Download
1 / 1
10 likes | 131 Views
Recovery-Oriented Systems of Care: An Examination of Recovery Support Service Types and Client Outcomes Laurel Mangrum, Ph.D. University of Texas at Austin, Addiction Research Institute. Results and Conclusions. Introduction. Client and Service Characteristics.

E N D
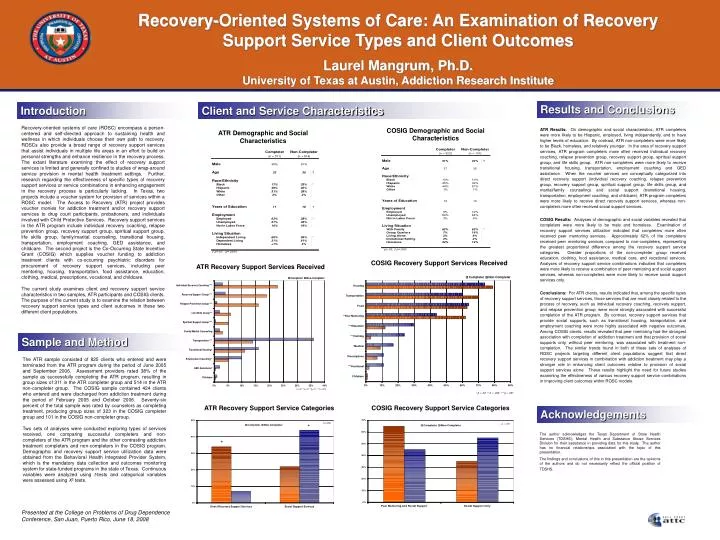
Recovery-Oriented Systems of Care: An Examination of Recovery Support Service Types and Client Outcomes Laurel Mangrum, Ph.D. University of Texas at Austin, Addiction Research Institute Results and Conclusions Introduction Client and Service Characteristics • ATR Results: On demographic and social characteristics, ATR completers were more likely to be Hispanic, employed, living independently, and to have higher levels of education. By contrast, ATR non-completers were more likely to be Black, homeless, and relatively younger. In the area of recovery support services, ATR program completers more often received individual recovery coaching, relapse prevention group, recovery support group, spiritual support group, and life skills group. ATR non-completers were more likely to receive transitional housing, transportation, employment coaching and GED assistance. When the voucher services are conceptually categorized into direct recovery support (individual recovery coaching, relapse prevention group, recovery support group, spiritual support group, life skills group, and marital/family counseling) and social support (transitional housing, transportation, employment coaching, and childcare), ATR program completers were more likely to receive direct recovery support services, whereas non-completers more often received social support services. • COSIG Results: Analyses of demographic and social variables revealed that completers were more likely to be male and homeless. Examination of recovery support services utilization indicated that completers more often received peer mentoring services. Approximately 62% of the completers received peer mentoring services compared to non-completers, representing the greatest proportional difference among the recovery support service categories. Greater proportions of the non-completer group received education, clothing, food assistance, medical care, and vocational services. Analyses of recovery support service combinations indicated that completers were more likely to receive a combination of peer mentoring and social support services, whereas non-completers were more likely to receive social support services only. • Conclusions: For ATR clients, results indicated that, among the specific types of recovery support services, those services that are most closely related to the process of recovery, such as individual recovery coaching, recovery support, and relapse prevention group, were more strongly associated with successful completion of the ATR program. By contrast, recovery support services that provide social supports, such as transitional housing, transportation, and employment coaching were more highly associated with negative outcomes. Among COSIG clients, results revealed that peer mentoring had the strongest association with completion of addiction treatment and that provision of social supports only, without peer mentoring, was associated with treatment non-completion. The similar trends found in both of these sets of analyses of ROSC projects targeting different client populations suggest that direct recovery support services in combination with addiction treatment may play a stronger role in enhancing client outcomes relative to provision of social support services alone. These results highlight the need for future studies examining the effectiveness of various recovery support service combinations in improving client outcomes within ROSC models. Recovery-oriented systems of care (ROSC) encompass a person-centered and self-directed approach to sustaining health and wellness in which individuals choose their own path to recovery. ROSCs also provide a broad range of recovery support services that assist individuals in multiple life areas in an effort to build on personal strengths and enhance resilience in the recovery process. The extant literature examining the effect of recovery support services is limited and generally confined to studies of wrap-around service provision in mental health treatment settings. Further, research regarding the effectiveness of specific types of recovery support services or service combinations in enhancing engagement in the recovery process is particularly lacking. In Texas, two projects include a voucher system for provision of services within a ROSC model. The Access to Recovery (ATR) project provides voucher monies for addiction treatment and/or recovery support services to drug court participants, probationers, and individuals involved with Child Protective Services. Recovery support services in the ATR program include individual recovery coaching, relapse prevention group, recovery support group, spiritual support group, life skills group, family/marital counseling, transitional housing, transportation, employment coaching, GED assistance, and childcare. The second project is the Co-Occurring State Incentive Grant (COSIG) which supplies voucher funding to addiction treatment clients with co-occurring psychiatric disorders for procurement of recovery support services, including peer mentoring, housing, transportation, food assistance, education, clothing, medical, prescriptions, vocational, and childcare. The current study examines client and recovery support service characteristics in two samples, ATR participants and COSIG clients. The purpose of the current study is to examine the relation between recovery support service types and client outcomes in these two different client populations. COSIG Demographic and Social Characteristics ATR Demographic and Social Characteristics COSIG Recovery Support Services Received ATR Recovery Support Services Received Sample and Method The ATR sample consisted of 825 clients who entered and were terminated from the ATR program during the period of June 2005 and September 2006. Assessment providers rated 38% of the sample as successfully completing the ATR program, resulting in group sizes of 311 in the ATR completer group and 514 in the ATR non-completer group. The COSIG sample contained 424 clients who entered and were discharged from addiction treatment during the period of February 2005 and October 2006. Seventy-six percent of the total sample was rated by counselors as completing treatment, producing group sizes of 323 in the COSIG completer group and 101 in the COSIG non-completer group. Two sets of analyses were conducted exploring types of services received, one comparing successful completers and non-completers of the ATR program and the other contrasting addiction treatment completers and non-completers in the COSIG program. Demographic and recovery support service utilization data were obtained from the Behavioral Health Integrated Provider System, which is the mandatory data collection and outcomes monitoring system for state-funded programs in the state of Texas. Continuous variables were analyzed using t-tests and categorical variables were assessed using X2 tests. ATR Recovery Support Service Categories COSIG Recovery Support Service Categories Acknowledgements The author acknowledges the Texas Department of State Health Services (TDSHS), Mental Health and Substance Abuse Services Division for their assistance in providing data for this study. The author has no financial relationships associated with the topic of this presentation. The findings and conclusions of this in this presentation are the opinions of the authors and do not necessarily reflect the official position of TDSHS. Presented at the College on Problems of Drug Dependence Conference, San Juan, Puerto Rico, June 18, 2008






