Download

1 / 28
280 likes | 443 Views
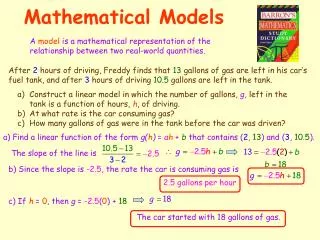
Mathematical Models for HIV-1 Therapy Optimisation. Mattia CF Prosperi, PhD ahnven@yahoo.it Clinic of Infectious Diseases Catholic University of Sacred Heart Largo F. Vito, 1 – 00168 - Rome, Italy. Summary. HIV-1 biology, treatment and resistance Epidemiology

E N D
Mathematical Modelsfor HIV-1Therapy Optimisation Mattia CF Prosperi, PhD ahnven@yahoo.it Clinic of Infectious Diseases Catholic University of Sacred Heart Largo F. Vito, 1 – 00168 - Rome, Italy
Summary HIV-1 biology, treatment and resistance Epidemiology Surveillance of resistance trends Phylogenetics, HIV-1 evolution Clustering of HIV-1 mutations Intra-host analysis HIV-1 replication, natural genetic drift and selective drug pressure Differential equation modelling Optimising treatments with machine learning Prediction of HIV-1 co-receptor usage Prediction of in vivo HIV-1 virologic response to treatments Genotype-based models Treatment history-based models Perspectives Modelling time to viral rebound, and resistance emergence Modelling epidemic with complex networks
HIV-1 epidemiology Usually focus on specific problems Incidence of new infections Temporal trends of treatment efficacy Determinants of virologic or immunologic failure … Standard models Univariable analysis (chi-square, t-test, rank-sum) Linear, logistic regression Survival analysis (Kaplan-Meier, Cox proportional hazard) Often limited when considering predictive ability of the models Complex Network models HIV-1 is peculiar! not only sexually transmitted, long asymptomatic stage, high rate of evolution, integration into host genome, no natural eradication, rapid development of drug resistance… SIR-like models, adjusted for MANY other factors like the drug resistance emergence (Smith, Blower et al., Science, 2010)
HIV-1 epidemiology (2) Several epidemiological studies carried out at our institute Temporal trends of drug resistance in Europe, considering different inhibition classes • We assessed the temporal trends of resistance by fitting a linear model, adjusting for potential confounders such as age, gender, mode of HIV transmission, introduction of new drugs…
HIV-1 phylogenetics Several scales of analysis Subtype evolution Transmission events (and drug resistance transmission) Note: phylogeneticanalysisconstructs a hierachyofsequencesthatrepresents the evolutionfromanhypotheticalancestor. Severaltechniques are available, fromdistance-basedclusteringtomaximumlikelihood, tobayesianclustering • Not always the phylogenetic reconstruction is able to trace the epidemiological evidence, due to sparse sampling (intra-host evolution does not proceed at a constant rate)
Howmuchdoestransmitteddrugresistancedependfromemergingdrugresistance?Howmuchdoestransmitteddrugresistancedependfromemergingdrugresistance? Probability of DR transmission intrinsic efficiency viral load frequency and modality of exposition
Large scale phylogenetics ≈12,000group M subtype B HIV-1 polymerasesequencescollectedfromItalian ARCA DB Maximum-likelihoodparallelphylogeny, computationally intensive Thereis no methodologyforautomatic cluster identification New techniqueforpartitioning a phylogenetictree Depth first visitwithconstraints on nodereliability and intra/inter-cluster patristicdistancedistributions Validated on a set ofknowntransmissionevents
Large scale phylogenetics (2) 11,541 sequences 9,855 patients Tree rooted on outgroup subtype J (ancient differentiation) 3D-hyperbolic geometry view Fractal dimension ≈1.6 Sustained level of differentiation
PrognosticFactorsofTransmissionClustering A more recent calendar year of sequencing Patients from central-Italy vs those from northern- or southern-Italy Heterosexuals and homosexuals vs injecting drug users Younger patients Patients with more recent infections (<4 years vs those infected >=14 years) Presence of resistance mutations in the protease gene
Clusteringof HIV-1 mutations Similar to phylogenetic analysis, but performed on transposed sequence alignments Useful to find associations among mutations under particular drug pressures Basis for structural analysis (Prosperi et al, ARHR 2009)
What’s going on in the body?Intra-hostmodelling System of differential equations Description of patient’s viral dynamics immune response Suitable for control theory (if equations could be treated analytically) Difficulties in dealing with prediction of therapy outcomes (see the constant ηvalues, indeedtheyshouldchange!) Difficulties modelling resistance outbreak (stochasticity, multi-strain models)
Accounting forviralevolution in differentialequations New approachto account bothfor treatment administration and viralevolution Stochasticmodelforviralnaturalevolution in absenceof treatment Calculationofinstantresistance at differenttimepointsusingin-vitroknowndrugsusceptibility Usageoftime-varyingresistance [η= η(t)] in the differentialequations and approximationwithnumericalsolutions Calculationofnumberofvirions in the nextreplication Selectionofresistantstrainswith roulette wheel procedure (fromgeneticalgorithmtheory)
Simulationresults Differentcombinationtreatmentsevaluated, alongwiththerapysequencingpolicies Althoughtheoreticallycomplex and sound, the modelwasnotsuitableforclinicalpractice (Prosperi et al, Bioinformatics 2008)
Restart:Optimisingtreatments We do notattempttodefineanexplicitmodel Extensiveuseofmachinelearning Linear and non-linearmodels Featureselection Robustvalidation In-vitro: predictionof HIV-1 co-receptorusage In-vivo: prediction of virological response to combination antiretroviral therapy (cART) Withviralgenotypic information Withoutviralgenotypic information Designedfor low/middle incomecountries
In-vitro: predictionof HIV-1 co-receptorusage HIV-1 can usetwodifferentco-receptors (CCR5/CXCR4) Entry inhibitors block only the CCR5 co-receptor The modelhelpsto decide if a patient can begivenan entry inhibitor or not, givenhisviralsequence Analysis using whole envelope region and other patient’s characteristics Logistic regression is a suitable model Notinferiortocomplexnon-linearmodels Performance (with robust validation) up to 93% accuracy 0.77 sensitivity 0.93 AUC (Prosperi et al, ARHR 2009)
In-vivo: prediction of virological response to cART Predicting the actual viral load changes following treatment switches is a challenging task Individual variability of immune response to infections add noise to the system Large number of possible therapeutic combinations leads to complex viral evolutionary pathways Other treatment-related factors such as pharmacokinetics and patient adherence to therapy play a crucial role in the control of virus replication and the development of resistance We focused on fixed patient’s follow up times (n-weeks of therapy)
Clinical and genomic data collection:The EuResistFoundation EuResist is a no-profit foundation (formerly EU-funded project), a consortium were hospitals, biology labs and universities cooperate Karolinskainstitute, Universityof Siena, UniversityofCologne, Max PlanckInstitute, IBM… It is the largest data base in the world comprising clinical, demographic and genomic data of HIV+ patients from national cohorts of Western Europe (at now Belgium, Italy, Germany, Sweden, Spain, Luxembourg) ≈34’000 patients ≈500’000 CD4 and ≈400’000 HIV-RNA measurements ≈100’000 antiretroviral therapies ≈31’000 HIV sequences (polymerase) Open to any kind of collaboration and data exchange
How to predict virological response for a given cART: study design Treatment Change Episodes (TCE) with a new cART Baseline HIV RNA load, CD4+ T cell counts Baseline HIV polymerase genotype and subtype Patient’s demographics (age, gender, ethnicity, mode of HIV transmission…) Previous drug usages (>1 year usage) for each drug class and each single drug 8-weeks and 24-weeks HIV RNA response Success defined as the achievement of <500 cp/ml (or >2 Log decrease from baseline at 8-weeks)
Treatment ChangeEpisode (TCE) The EuResist repository was queried and generated more than 3,000 TCE that were used for training and validating a prediction engine
Statistical learning models, feature selection and validation techniques Statisticallearningmodels LogisticRegressionwithhigher-orderinteractions (LR) AIC stepwiseselection RandomForests (RF) FeatureimportanceevaluationwithStrobl’s method Bayesiannetworks (BN) Three independentmodelsweremergedimproving performance Extra sample errorestimation Multiple ten-fold cross validation (MCV) Adjusted t-test on MCV performance distributionsformodelcomparison Externalindependent test set evaluation Comparisonagainsthumanexperts Comparisonagainstrule-basedalgorithms (Stanford, Rega, ANRS)
Customised cART sequencing The EuResistwebservice Statistical models Web-service Patient’s Age, gender HIV RNA CD4 Experienced drugs HIV genotype
Results The EuResist model outperforms the whole set of state-of-the-art techniques (i.e. rule-bases) and is as good as the world’s best human experts The average accuracy on validation is 76%, and AUC is 0.77 (Prosperi et al, Antivir Ther 2009)
Relaxing the need for a genotype:a perspective for cART optimisation in limited resource settings using therapy history In high-income countries, guidelines recommend genotypic resistance testing (GRT) both before starting antiretroviral therapy (ART) and at ART failure Appropriate funding and/or facilities to perform GRTs may be not available in low-middle income countries (LMIC), leaving physicians to switch therapy based solely on the clinical/immunological conditions (sometimes even without virological monitoring) Treatment history (TH) is one of the most crucial factors to play a role in the response to a new treatment. Other important factors are virologic and immunologic monitoring
Comparingmodelsusing GRT vs TH GRT-based vs TH-based models were compared to see if there were sensible loss in performance Performance of the model were tested in extra-EU-like scenarios Tests on a larger set of TCE without the mandatory GRT baseline attribute were carried out No statistically significant differences found by comparing GRT and TH models
Perspective We want to design and test a model that predicts viral load rebound over time using Patient’s viral genotypic information Patient’s clinical and demographic background • Suitable models: Cox regression, random survival forests • Need to define an appropriate goodness of fit • Preliminary inquire on the EuResist DB gave a considerable number of training instances
Perspective (2) Also, we might be interested in a model that predicts drug resistance emergence
Perspective (2) Design and test an epidemic model for HIV-1 using complex networks Start from Science paper and from other models presented in literature New insights Capability to handle dynamics at a regional, national and international level Effective description of Infection incidence over different risk group strata Homogeneous vs heterogeneous mixing? Drug resistance trends Prevision of trends with the introduction of new inhibition classes Prevision of HIV-1 evolution with respect to drug resistance prevalence in the treatment-naive population Account for transmitted drug resistance from treatment-naive and treatment-experienced patients How much shall we go into details as concerns the intra/inter-host genetic HIV-1 evolution?