Download
1 / 33
330 likes | 492 Views
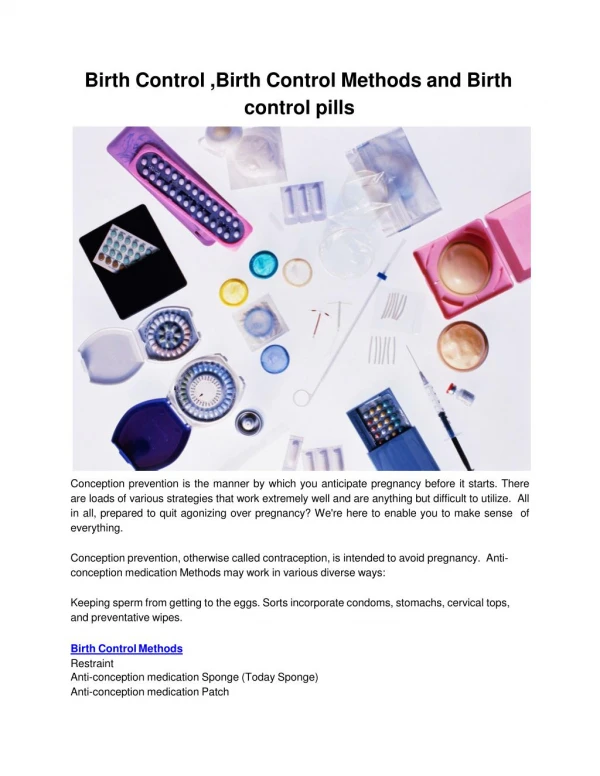
Birth. LABOUR: Complex mix of fetal signals and endocrine mechanisms in the mother. Fetus secretes surfactant protein which seems to alter maternal hormones.

E N D
Birth LABOUR: • Complex mix of fetal signals and endocrine mechanisms in the mother. • Fetus secretes surfactant protein which seems to alter maternal hormones. • Also, the agents (progesterone, nitric oxide, and others) that keep the uterine muscle quiet, decrease, and the uterus starts to contract. • sometimes timing is off premature labour
BIRTH LABOUR: • Surfactin signals mom’s hypothalamus: produced when fetal lungs ready to breathe
BIRTH LABOUR (Cont’d): • Hypothalamus stimulates pituitary • Pituitary secretes oxytocin • Oxytocin makes uterus contract: labour begins
BIRTH Other mechanisms involved in the start of labour: • CRH: corticotropin-releasing hormone: released by the placenta. Amounts correlate with date of labour (early, on time or post-dates) by the 16th-20th weeks gestation • CRH seems to trigger fetal production of cortisol. Cortisol clears fluid from infant’s lungs and stimulates more CRH production. This, in turn, stimulates placental estrogen production, necessary for starting labour.
BIRTH SOME POSSIBLE SIGNS OF LABOUR: • Mucus plug falls out from cervix • Amniotic fluid leaks or gushes out • Contractions - but … Braxton Hicks: False Labour
BIRTH STAGES OF LABOUR: • “False” labour: Braxton-Hicks contractions • First stage: • early first stage: longest (hours or days), mild contractions, 10-30” duration @ 20, 15, 10, 5’ intervals • late first stage: 60-90” duration @ 3, 2, 1’ • transition: shortest, (15-30’) most intense, random pattern of contractions. • All along, cervix dilating and effacing (thinning)
BIRTH STAGES OF LABOUR (Cont’d): • Second stage: • cervix fully dilated (10 cm) • baby moves down birth canal • crowning • duration: primiparas about 1 hr., multiparas faster • head first, rotation • shoulders, one at a time • rest of baby slithers out
BIRTH STAGES OF LABOUR (Cont’d): • Third stage: • after 10-15’ interval • expulsion of placenta • During interval between stages 2 and 3: • lungs start to work gradually • cord delivers last of maternal blood to infant • heart valves close • cord must not be cut until white and not pulsing
BIRTH • Birth: • empowering experience for mother • Super-orgasm (Kitzinger) • Gentle pushing, breathing baby out • Mouth open leads to open introitus
BIRTH POSITIONS FOR LABOUR • Not on her back!!! Lithotomy Position • Weight of uterus and its content on abdominal aorta: can cause reduced blood flow to fetus • Slows down labour • Importance of gravity’s help
BIRTH POSITIONS FOR BIRTH • Standard: lithotomy – one of the worst. Better: • sitting up reclined • lying on her side • on hands and knees • Unmedicated, undisturbed birth best. 90-95% births do not need intervention.
BIRTH RISKS OF INDUCING LABOUR: • Contractions too hard, lead to more analgesics and anesthetics • Hard contractions can also lead to uterine rupture and to brain damage (pressure on the skull) • If lungs not ready, leads to respiratory distress (formerly called hyaline membrane) due to lack of surfactin
Placenta praevia Classification and external resources BIRTH POSSIBLE COMPLICATIONS (5-10%) • inefficient placenta, affects fetal growth, life threatening for fetus • placenta previa Diagram showing placenta praevia. ICD-10 044, P02.0 ICD-9 641.0, 641.1 MeSH D010923
BIRTH POSSIBLE COMPLICATIONS (5-10%) • abruptio placenta • transverse presentation • breech presentation (feet or buttocks) • prolapsed cord • cord pinched or wrapped around neck
BIRTH POSSIBLE COMPLICATIONS (5-10%) (Cont’d): • small pelvic diameter • multiple births • toxemia: elevated BP, fluid retention, can lead to eclampsia (possibly fatal) • maternal asthma
BIRTH POSSIBLE COMPLICATIONS (5-10%) (Cont’d): • All carry risk of hypoxia or anoxia • Hypoxia: • reduced oxygen • Anoxia: • NO oxygen • Consequences: • brain damage • detectable or subclinical
BIRTH POSSIBLE IATROGENIC EFFECTS OF INTERVENTION: Common interventions: • Induction of labour (pitocin), use of pitocin to re-start or accelerate labour: can cause too strong contractions, pain, uterine rupture. Due date myth. • Episiotomy (infections, painful sex, painful sitting)
BIRTH POSSIBLE IATROGENIC EFFECTS OF INTERVENTION: Common interventions (Cont’d): • C-section: major abdominal surgery; possible lack of adrenaline/noradrenaline in baby. N. American C-sec rates too high • Psychosocial factors: • vagina preservation • no pain or awareness • set the date
BIRTH POSSIBLE IATROGENIC EFFECTS OF INTERVENTION: Common interventions (Cont’d): • Medical factors: • ultrasounds • fetal monitors • higher maternal age • tummy tuck combined with C-section • Pain medication (analgesics and anesthetics): can slow down labour and decrease oxygen delivery to baby
BIRTH POSSIBLE IATROGENIC EFFECTS OF INTERVENTION: Common interventions (Cont’d): • Fetal monitor: external or internal • External: curtails movement, mother on her back • Internal: possible damage to baby, also curtails mother’s movement • Forceps • All interventions potentially iatrogenic: damage caused by medical treatment.
BIRTH EFFECTS OF ANESTHETICS AND ANALGESICS: • slow down labour (leading to pitocin use) • sluggish baby • mother zonked, weak • can interfere with bonding • can interfere with lactation • can interfere with rooming-in
BIRTH SOME POST-NATAL EFFECTS OF HYPOXIA • Increased SIDS • Increased risk of respiratory illnesses • Weaker sucking reflex • Weaker head-turning reflex • Increased hyperactivity • Increased difficulty in reading and math
BIRTH BIRTH HORMONES (INFANT) • Adrenaline and noradrenaline • open airways, lungs • enhance cell metabolism • more blood to brain • alertness • Not released in C-section
BIRTH BIRTH HORMONES (INFANT) • Could be interfered with when administering drugs to mother during labour • No thorough longitudinal study but 80% increased risk of asthma by age 8 • Silver nitrate, drops in baby’s eyes in case of maternal gonorrhea (blindness) but… • Interferes with bonding, can be delayed an hour
BIRTH • In some cultures, intercourse used to start or accelerate labour. • How soon can have sex post-partum? Six weeks or when ready. Effect of episiotomy, C-section. • Moms who breastfeed tend to return to sex earlier. Results depending on sampling and methodology. In both parents testosterone decreases, prolactin increases. • Tiredness, lack of sleep, overwhelmed • Change in roles, decrease of “romanticism”.