Download
1 / 64
640 likes | 673 Views
Explore the significance of the Mauve Factor (OHHPL) in identifying oxidative stress related to behavioral disorders. Discover its history, association with stress, and treatment correlations. Learn about symptoms, levels, and the impact on conditions like Down syndrome, autism, and schizophrenia.

E N D
Urinary pyrrole (Mauve Factor): marker for oxidative stress in behavioral disorders Woody McGinnis MD mcginnis@mind.net Seattle, 6 November 2004
The Mauve Factor CH3 C2H5 OHHPL (hydroxyhemopyrrolin-2-one)
OHHPL (Mauve Factor) • In human urine, blood and CSF • Mistakenly identified as kryptopyrrole, a persistent erroneous term • Chemically similar to kryptopyrrole, which can be used for OHHPL assay
HP KP CH3 C2H5 C2H5 CH3 OHHPL OHKPL CH3 C2H5 C2H5 CH3
Mauve history • Discovered in urine in 1957 • Named for lilac-colored appearance on paper chromatograms developed with Erhlich's reagent • Labile and elusive • Abram Hoffer is the father of Mauve
Hoffer Irvine Osmond Pfeiffer Sohler Cutler O'Reilly Graham Riordan Jackson Walsh Audhya Europe Mauve Hall of Fame
Hoffer J Neuropscyh 1961 • Qualitative Mauve assay • All normals mauve-negative • 27/39 early schizophrenics positive • All 7 who recovered on niacinamide converted to negative
Hoffer 1961 • Relapses associated with reappearance of Mauve • Apparent role in other behaviors: ETOH, depression. • A "mentally retarded" mauve-positive child responded dramatically to niacinamide
Hoffer and Mauve • Heat and light sensitive • Relatives should be tested • Preventive potential • 10/14 criminal / deviant positives • Report on 740 patients in 1966 • All recovered schizophrenics negative, unrecovered 50% positive
O'Reilly 1965 • Report on 850 behavioral patients • 25% of "disturbed children" mauve-positive, vs 12% of well children • First documented observation of Mauve association with stress
Mauve in schizophrenia • Hoffer 1961, 1963, 1966 • Yutwiller 1962 • O'Reilly 1965 • Sohler 1967 x 2
High-Mauve and behavior • Down syndrome 70% • Schizophrenia 40-70% • Autism 50% • ADHD 30% • ETOH 20-80%
Carl Pfeiffer 1972 • "Sara" 15 y.o. with four years of unreality spells, insomnia, seizures, attempted suicides, knee problems; quite well on B6 1000 mg, Zn 160 mg, Mn 8 mg. • Signs, symptoms, and clinical response imply high B6 / zinc need in high-Mauves. • B6 and zinc quickly recognized by clinicians as main-stay treatment.
Mauve levels • Clinicians: behavioral symptoms in individuals correlate with level • Irvine 1972: likelihood of depressive reactions correlate with level • Cutler 1974: B6 dose needed to normalize Mauve proportional to level • McCabe 1983: Mauve can be normalized with high-dose B6 only
Pfeiffer 1983 • Symptoms may improve in 24 hours, usually within 1 week • May need months for full recovery • Relapse within days or weeks if no nutrients • Changing needs
OHHPL Levels and B6 (10mg/kg/day) + Zn (25mg) + Mg (400mg) in Autism
Nail spots Stretch marks Pale skin Poor tanning Knees and joints Constipation Dream recall Morning nausea Light and sound Odor intolerance Migraines Stitch-in-side Pfeiffer correlates
Walsh Low stress tolerance Anxious, overly pessimistic Explosive anger Hyperactivity Kruesi Social withdrawal Emotionally labile Loss of appetite Fatiguability
Mauve and stress • Mauve is associated with stress, including, emotional stress. Audhya 1992. Cold-immersion increased Mauve <1 hour • The correlation is well-documented over decades
Mauve and stress O'Reilly 1965 Sohler 1971 Pfeiffer "stress-dosing" 1973 Ward says across all diagnoses 1975 Hippchem 1978 McCabe 1983 Jaffe and Kruesi 1992
Non-behavioral Mauve • Acute Intermittent Porphyria • Cutler 1974: High-mauve obesity and abnormal glucose tolerance • Hoffer 1966: 33/99 Cancer patients, 7/8 lung cancer patients • Riordan and Jackson: 43% of general medical patients: arthritis, chronic fatigue, heart disease, hypertension, irritable bowel, migraine. Range 20-40 mcg%.
Mauve bumps in the road • U Michigan 1962: no pathological importance in schizophrenia because found 34% Mauve-negative. • U Cal 1969: their "simplified" assay produced phenothiazine false-positive • India 1971: No Mauve in 120 psych patients--used HCl, 24° collection.
More bumps in the road.. • Am J Psychiatr 1978: "Pyroluria a poor marker in chronic schizophrenia" (based on 2/9 Mauve-positives) • J Nutr 1979: "..urinary kryptopyrrole..proved invalid as screening test for vitamin dependent disorders.." (based on 6/20 Mauve-positives, all borderline. And no zinc.)
Bumps • U Cal 1975: "Non-occurrence of kryptopyrrole and hemopyrrole in urine of schizophrenics by GC-MS" • UC Berkeley 1978: GC/MS shows no kryptopyrrole or hemopyrrole in schizophrenics or controls • Irvine 1977-78 confirms Mauve is OHHPL by synthesis.
Bumps.. • Irvine, Nature 1969: Mauve identified unequivocally as kryptopyrrole • Irvine, in landmark OrthomolecularPsychiatry, "Mauve is kryptopyrrole" • Irvine 1974: lactam of kryptopyrrole is the "identity of the natural kryptopyrrole"
Was Pfeiffer right about Mauve and low zinc? Walsh. 1148 ADHD patients: Plasma Zn vs colorimetric Mauve Strong negative correlation 0.974 significance (F test)
OHHPL vs. RBC Zinc Correlation Coefficient -.985
Mauve vs WBC Zinc Correlation Coefficient -.743
Mauve as clinical tool • Careful specimen collection • Mild 20-30, moderate 30-40, severe over 40 mcg% • Elevations imply zinc and B6 need • Titrate nutrients to suppress Mauve • Individualize adjunctive nutrients
Mauve is OHHPL • Graham, Univ Glasgow 1978 quantified normal range by GLC • Audhya 1994-present: commercial OHHPL by HPLC/MS and synthetic standard. • Strong logical imperative to cease "kryptopyrrole" terminology
OHHPL facts • Irvine 1977: levels correlate with emotional withdrawal, motor retardation, blocked affect and severe depression; IP to rats: ptosis, locomotor aberration, hypothermia • Cutler 1990: IP to mice increased backward locomotion and head-twitching (as with psychotomimetics)
OHHPL facts • Photo, heat, and acid-labile • Urinary half-life 10-12 hours • Nearly 100% urinary clearance intact after IP administration • Daily excretion up to 1 mg • Urine, Blood, CSF; animal brain • Graham: similarity to kainic acid and pyroglutamate suggests excitoxicity
Why do they both work? Niacinamide (B3) OR Vitamin B6 (P5P) and Zinc
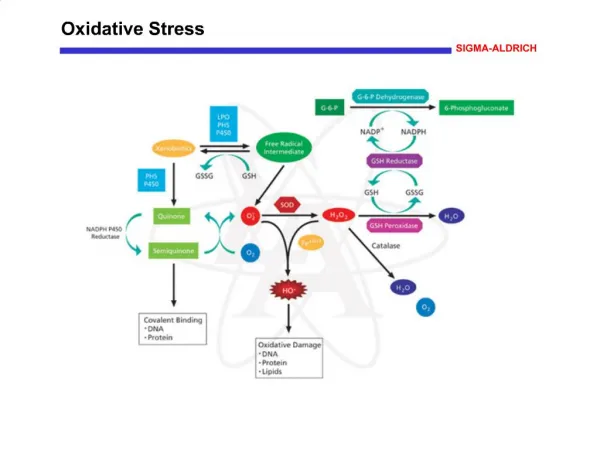
Thinking points • B3, Zn and B6 are anti-oxidant • Strong stress / Mauve association • Emotional stress clearly causes oxidative stress • The behavioral and somatic high-Mauve disorders feature high oxidative stress
High Oxidative Biomarkers • Down Syndrome • Schizophrenia • Autism • ADHD • Emotional Stress • Cancer and Inflammatory Disease • Hyperglycemia
Zinc is anti-oxidant • Shields -SH groups • Blocks lipid peroxidation and PLA2 • Induces metallothionein • Constituent of SOD • Maintains vitamin A • Deficiency increases intestinal NO˙
Zinc deficiency increases oxidative stress • Lower glutathione, vitamin E, GST, GSHPx and SOD • Increased reactive species and lipid peroxides in tissue, membranes and mitochondria
Oxidants mobilize zinc • Oxidants release complexed zinc from zinc-binding proteins, including metallothionein and albumin • It is likely--but unproven--that zinc retention is reduced in direct relationship to oxidative stress
Oxidative stress Low zinc
B6 is anti-oxidant • P5P for Glutathione, Metallothionein, CoQ10 and Heme synthesis • With Zn, cofactor for GAD • P5P protects vulnerable lysinyl groups, as in GSHPx
Marginal B6 deficiency: Lowers GSHPx Lowers glutathione reductase Promotes mitochondrial decay Raises lipid peroxide levels
B6 and oxidative stress • Binding of P5P-dependent enzymes is subject to carbonyl inhibition • Binding of key P5P-dependent enzymes such as GAD impaired by oxidants generally • OH˙ and 1O2 attack B6 vitamers
B6 and Mauve • B6 levels are normal • Pfeiffer alluded to lower P5P and EGOT activity in high-Mauves • Lower zinc may impair B6 activation • Oxidative stress affects activation of B6 and binding of B6-dependent enzymes
B3 is anti-oxidant • NADPH for reduction of glutathione • Potent free-radical quencher: protects both lipids and proteins from oxidation • Blocks NO˙ neurotoxicity • High tissue levels: better lipoxidation prevention than ascorbate
B3 is anti-oxidant • Niacin antagonists increase lipoxidation • Low B3 decreases MT and increases apoptosis in brain cells • Neuroprotective in experimental mitochondrial toxicity
Reciprocal relationships Oxidative stress Poor energeticsExcitotoxicty
Cystathionine synthase Catalase Heme-hemopexin for MT translation Pyrrolase Guanylate cyclase Cytochromes Sulfite reductase NOS Require heme