Download
1 / 17
170 likes | 325 Views
Lecture 2. Information processing and intuitive decision making theory Carl Thompson. Decision making theory. Descriptive approaches: how people actually make decisions Normative approaches: how people ought to make decisions NB. Most approaches have elements of both.

E N D
Lecture 2 Information processing and intuitive decision making theory Carl Thompson
Decision making theory • Descriptive approaches: how people actually make decisions • Normative approaches: how people ought to make decisions • NB. Most approaches have elements of both
Information processing • Assumptions • Human reasoning as the interface between short (stimuli) and long-term (semantic/factual knowledge & experiential (episodic knowledge) memory • Human reasoning is rational • Rationality is bounded
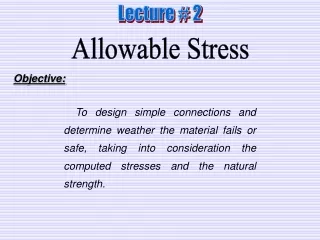
Elstein et al. 1978 Cue acquisition H° generation Cue interpretation H° evaluation Carnevali et al 1984 Exposure to pre-encounter data Entry to the data search field and shaping data gathering Coalescing cues into chunks Activating possible H° H° directed search of the data field Testing H° Dx Information processing: the process
he could not take the sleeping tablets as he could not swallow…. the DN said that they might have to put up a syringe driver for the night if he was not settling and could not take anything orally. ….. he had a couple of dressings on his bottom and the dressings were intact. The DN decided to leave them and not to move him around too much as he had not slept much that night….. ……she told her that it would not be long until he died…… his breathing would get shallower, occasionally it would seem as though he would not breathe again…..it showed that he was nearer to dying…… the DN said that the Marie Curie nurses could work for up to 27 hours and she thought that it would be better if they came at night …..she would return in the afternoon to reassess him
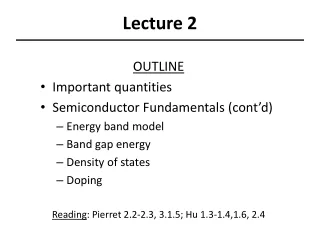
Information cues Signs and symptoms Optimal judgement Test results Nurses’ Judgements Patient preferences Etc. Brunswik’s lens model
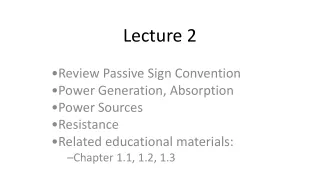
Importance Utility(s.e.) Factor öòø SYSTOLIC systolic BP 4.59 óó 3.4298(9.3211) ó- normal õò÷ -2.9035(9.3211) -ó equivocal ó -.5263(8.9352) ó abnormal ó öòòòòòòòòòø PULSE pulse ó26.80 ó 18.5965(9.3211) ó---- normal õòòòòòòòòò÷ -18.404(9.3211) ----ó equivocal ó -.1930(8.9352) ó abnormal ó öòòòòø RESPS resps 13.13óó -5.0702(9.3211) -ó normal õòòòò÷ -6.5274(8.9598) -ó equivocal ó 11.5976(8.9598) ó-- abnormal ó öòòòòø O2 oxygen sats 14.73óó -12.070(9.3211) ---ó normal õòòòò÷ 8.2632(9.3211) ó-- equivocal ó 3.8070(8.9352) ó- abnormal ó öòòòòòòòø URINE urine output ó21.64 ó 11.6393(8.9598) ó--- normal õòòòòòòò÷ 6.5965(9.3211) ó- equivocal ó -18.236(8.9598) ----ó abnormal ó öòòòòòòø GCS glasgow coma score ó19.11 ó -7.5702(9.3211) --ó normal õòòòòòò÷ -9.4035(9.3211) --ó equivocal ó 16.9737(8.9352) ó---- abnormal ó 53.5702(6.5013) CONSTANT Pearson's R = .838 Significance = .0000 Kendall's tau = .570 Significance = .0003 Summary of judgement policy for one clinician faced with the Dx of shock in critical care. Utilities Importance Internal consistency
Other health information: smoker? Mobility? Medication?…etc General medical condition: diabetic? RA; anaemic?… etc ARTICLES DAILY VISITS Doppler ABPI Compliance? History: how and when ulcer started; current treatment; pain… etc PHYSIOLOGY Ulcer: size, odour, slough, exudates? Background information Investigations: urine, FBC, ESR, urea and electrolytes, blood glucose, swab (if appropriate) Leg exam: oedema, temperature; ankle and calf circumference… PATIENT INFORMATION COLLEAGUE’S ‘EXPERIMENTS’ general condition: well? Pulse, BP, weight COST PATIENT REJECTION OF EXPERTISE ROLE CONFLICT, GP WISHES REJECTION OF EXPERTISE CNS NEED FOR VISIBILITY IN DECISION SHARED DECISION MAKING VALUES SEEING IS BELIEVING AND EXPERIMENTATION WOUND FORMULARY COST DOWN TO WHAT I’VE USED OVER THE YEARS
Problems with info processing • Role of H° • Over emphasising positive findings • Excessive data collection
Intuition and expertise • Understanding without a rationale (Benner & Tanner 1987 p2) • A perception of possibilities, meanings and relationships by way of insight (Gerrity 1987 p63) • Knowledge of a fact or truth, as a whole; immediate possession of knowledge; and knowledge independent of the linear reasoning process (Rew and Barron 1987 p60) • Immediate knowing of something without the conscious use of reason (Schrader and Fischer 1987 p45) • [A] process whereby the nurse knows something about a patient that cannot be verbalised, that is verbalised with difficulty or for which the source of knowledge cannot be determined (Young 1987 p52)
Intuition • Type of knowledge vs mode of thought • Lack of visibility • Dubious morality? • Reflective ‘paradox’ and ?black box • Accurate sometimes (hindsight?) • Lack of power
Novice - expert • Dreyfus’ and Benner • Novice • Advanced beginners • Competent • Proficient • Expert
performance • Whole situation • Orientation • Decision • Situation components • Perception • action
‘the rules’ • Realise that expertise is acquired step-by-step • Avoid trying to think like an expert (intuitively) • Practice intensively using the rules and logic that are available • *NB the proponents’ discipline (sociology/naturalistic research) does not demand empirical testing so caution advised
Points of contact and divergence • Communicability • Simplification • Context specificity • applicability