Download
1 / 26
260 likes | 416 Views
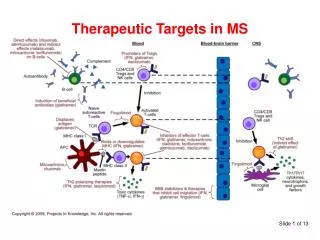
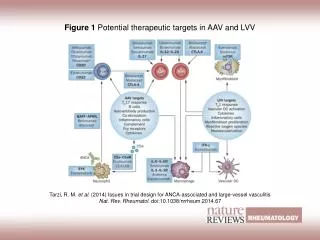
Possible Biomedical Informatics pilot study Integration of viral genomics with clinical data in HIV infection. Present therapeutic targets in HIV life cycle. ATTACHMENT. Nucleoside RT Inhibitors (NRTI). FUSION. Fusion inhibitors. Non-nucleoside RT inhibitors (NNRTI). UNCOATING.

E N D
Possible Biomedical Informatics pilot studyIntegration of viral genomics with clinical data in HIV infection
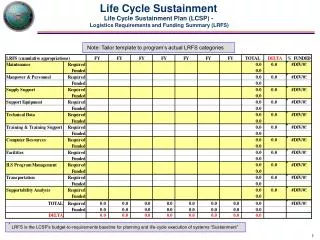
Present therapeutic targets in HIV life cycle ATTACHMENT Nucleoside RT Inhibitors (NRTI) FUSION Fusion inhibitors Non-nucleoside RT inhibitors (NNRTI) UNCOATING REVERSE TRANSCRIPTION INTEGRATION TRANSLATION TRANSCRIPTION Protease inhibitors (PI) EXPORT MATURATION RELEASE VIRUS ENZYMES 20 drugs in 4 drug classes
Major steps in antiretroviral therapy • 1987-1991: monotherapy (AZT or ddI) Limited and transient effect (low potency, resistance, toxicity) • 1992-1995: ‘dual’therapy (e. g. AZT+ddI, AZT+ddC, AZT+3TC) Increased efficacy but still unable to control HIV replication • 1996-present: ‘triple’therapy (2 NRTI + 1 PI) Highly potent regimens, long-term suppression of viral replication to undetectable levels but virus eradication still unachievable Combination therapy (3-4 drugs) Highly-active antiretroviral therapy (HAART) Decrease in HIV mortality in association with PI-based combination therapy (Palella, NEJM 1998)
HAART ‘Suppression’ of viral replication (HIV genome undetectable in plasma) however… Persistence of HIV in different reservoirs (CNS, lymph nodes, genital tract, macrophages) Latent infection / Chronic infection thus… Eradication of HIV is not currently achievable HAART is a long-term, possibly lifelong treatment Medium-term and long-term toxicity, adherence issues
Causes for antiretroviral treatment failure POOR ADHERENCE LIMITED POTENCY TREATMENT FAILURE POOR PHARMACOKINETICS DRUG RESISTANCE
POOR PHARMACOKINETICS POOR ADHERENCE LIMITED POTENCY DRUG RESISTANCE Causes for antiretroviral treatment failure TREATMENT FAILURE
Global picture of antiretroviral resistance (Patients under HAART in developed countries) • Resistance to drugs of a single class NRTI 50-70%, NNRTI 35-45%, PI 35-55% • Resistance to drugs of all three classes (MDR) 5-25% • Resistance to any drug in newly infected subjects (“transmitted resistance”) 5-25%
Antiretroviral resistance testing in clinical practice (as recommended by the International AIDS Society 2001-2003) • At treatment failure To guide treatment switch • Before starting treatment To detect transmitted resistance • Pregnancy To reduce mother-to-child transmission
Publications on antiretroviral drug resistance No. of papers Medline search: ‘HIV drug resistance’, [only items with abstracts] • International HIV drug resistance workshop (yearly) • European HIV drug resistance workshop (yearly) • Dedicated session at all major international HIV & Infectious Diseases conferences
How to measure response to treatment? ‘Viral load’ (plasma HIV RNA) CD4/mm3 600 500 400 300 200 100 HIV RNA levels and CD4 counts are the reference surrogate markers for monitoring response to treatment
PCR product(s) Plasma RNA Cloning into or recombination with a lab-adapted backbone Recombinant virus In vitro drug susceptibility assay How to measure antiretroviral resistance? Option 1. PHENOTYPE: culture HIV in the presence of increasing doses of each antiretroviral drug and quantitate virus replication
How to measure antiretroviral resistance? Option 1. PHENOTYPE: culture HIV in the presence of increasing doses of each antiretroviral drug and quantitate virus replication • Calculates fold-resistance level (i. e. amount of drug needed to stop patient virus replication with respect to reference wild-type virus) • Translation of fold-resistance levels into clinically relevant categories (i. e. sensitive vs. resistant) not straightforward: “clinical cut-offs” vary from 1.4-fold to >10-fold for different drugs • Technically demanding: cumbersome, lengthy, difficult to standardize • Assay available from two specialized companies (Virco, ViroLogic) at high cost • Important for formal characterization of drug resistance mutations but definitely not suitable for routine application
A C G T How to measure antiretroviral resistance? Option 2. GENOTYPE: sequence the relevant part of HIV genome and infer the drug susceptibility profile based on the mutations detected and known genotype-phenotype correlations PCR product(s) Plasma RNA Cycle sequencing reactions Automated sequencer Genotype interpretation
How to measure antiretroviral resistance? Option 2. GENOTYPE: sequence the relevant part of HIV genome and infer the drug susceptibility profile based on the mutations detected and known genotype-phenotype correlations • Predicts categorical levels (e. g. susceptible, intermediate, resistant) • Complex and/or rare mutational patterns difficult to interpret • Technically easier: no virus culture, faster turnaround time, amenable to full automation • Assay available from several molecular diagnostics companies (some FDA-approved for in vitro diagnostic use). Home-brew systems can be developed and used successfully • Many computerized interpretation algorithms, updated regularly by ‘expert panels’. However, different algorithms may yield different results on the same sequence, particularly for certain drugs
Drug resistance mutations gp41 200 bases (?) PR RT 1,300 bases
Antiretroviral resistance testing PHENOTYPE Virus cultivation in the presence of drugs In vitro fold-resistance CUT-OFF (??) GENOTYPE PREDICTION of response to treatment and choice of the best drugs Detection of mutations in HIV genome
A novel approach: from genotype to treatment response PREDICTION of response to treatment and choice of the best drugs GENOTYPE
A novel approach: from genotype to treatment response CD4 Treatment switch HIV RNA Baseline GENOTYPE Follow-up data Model training (e. g. neural network, genetic algorithms)
INPUT OUTPUT ‘Virtual response’ model Input data RT GENOTYPE 41L 210W 215Y PR GENOTYPE 10I 63P 77I 90M HIV RNA4.3 log CD4330 Treatment AZT, D4T+DDI+EFV Predicted response at 6 months Regimen 1 - 1.5 log HIV RNA +126 CD4 Regimen 2 - 1.3 log HIV RNA +102 CD4 ..….. ..….. Computation Public Server Remote user
Is this topic suitable for a BMI strategy? • Inadequacy of the present tools: both phenotyping and genotyping have been shown to be useful in the clinic but there is still much to improve • Complexity of the virus: lots of mutations, “quasispecies” nature of HIV population within an individual • Complexity of treatment: 4 drug classes, 3-4 drugs in a typical regimen, new drugs and drug classes in the pipeline • Standard quantitative indicators as output variables: HIV RNA levels and CD4 cell counts • Amount of data: tens of thousands of HIV sequences generated in Europe each year • Availability of data: HIV sequence data stored in the lab, treatment and follow-up data stored in the clinic
Linear Regression Analysis(based on updated neural network model)
ARCA (Antiretroviral Resistance Cohort Analysis)https://www.hivarca.net
ARCA - Partecipating clinical and lab units (April 2004) Some centers in the region All the centers in the region ~3.500 patients ~12.000 HIV sequences