Download
1 / 51
550 likes | 797 Views
MECHANISM OF MUSCLE CONTRACTION. Ginus Partadiredja The Department of Physiology UGM, Yogyakarta. Muscle = neuron excited chemically, electrically, mechanically to produce action potentials Muscle neuron contractile mechanism activated by action potentials. Skeletal muscle:

E N D
MECHANISM OF MUSCLE CONTRACTION Ginus Partadiredja The Department of Physiology UGM, Yogyakarta
Muscle = neuron excited chemically, electrically, mechanically to produce action potentials • Muscle neuron contractile mechanism activated by action potentials
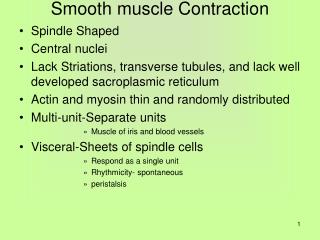
Skeletal muscle: • cross-striations • does not contract without innervation • lacks anatomic & functional connections between fibers • voluntary control • Cardiac muscle: • cross-striations • functionally syncytial • contracts rhythmically in the absence of external innervation • contains pacemaker • Smooth muscle: • Lacks cross-striations • functionally syncytial • contains pacemaker
Skeletal muscle muscle fibers myofibrils • Muscle fiber: multinucleated, long, cylindrical, single cell surrounded by sarcolemma (cell membrane)
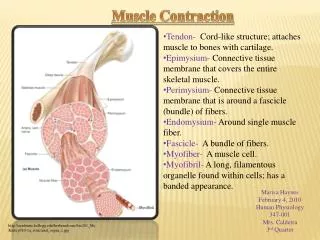
Filaments = contractile proteins: • Myosin II (thick filament) • Actin • Tropomyosin • Troponin: - Troponin I thin filament • - Troponin T • - Troponin C
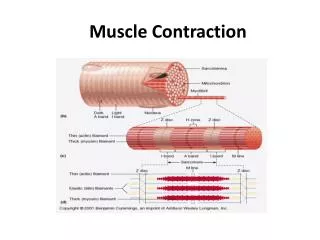
Thick filaments A bands Thin filaments I bands
Myosin 2 globular heads & long tail • Head of myosin contains actin-binding site & catalytic site that hydrolize ATP
Thin filaments two chains of actin • Tropomyosin in the groove of actin • Troponin: T binds other troponin to tropomyosin • I inhibits the interaction of myosin & actin • C contains the binding sites for Ca+2
Sarcotubular system = T system + sarcoplasmic reticulum • T system of tubules + adjacent terminal cisternae = triad • T system rapid transmission of action potentials from the cell membrane to the fibrils
The resting membrane potential of muscle = -90 mV • The action potential = 2 – 4 ms • The speed along the muscle = 5 m/s • The absolute refractory period = 1 – 3 ms • The distribution of ions nerve cells • Depolarization = Na+ influx • Repolarization = K+ efflux • Depolarization starts at motor end plate transmitted along the fiber contractile response
Sequence of events during transmission from the motor nerve the muscles = transmission in synapses between neurons
Sequence of Events in Contraction and Relaxation of Skeletal Muscle Steps in Contraction: 1. Discharge of motor neuron end of motor neuron Ca+2 enters the endings
2. Release of transmitter (acetylcholine) at motor end-plate 3. Binding of acetylcholine to nicotinic acetylcholine receptors (concentrated at the tops of the junctional folds)
Increased Na+ and K+ conductance in end-plate membrane • Generation of end-plate potential • Generation of action potential in muscle fibers
7. Inward spread of depolarization along T tubules excitation – contraction coupling 8. Release of Ca+2 from terminal cisterns of sarcoplasmic reticulum and diffusion to thick and thin filaments
9. Binding of Ca+2 to troponin C, uncovering myosin-binding sites on actin (at resting, troponin I is tightly bound to actin and tropomyosin covers the sites where myosin heads bind to actin) • ATP is then split ADP + Pi contraction
10. Formation of cross-linkages between actin and myosin and sliding of thin on thick filaments, producing movement
Steps in Relaxation: • Ca+2 pumped back into sarcoplasmic reticulum diffuses into the terminal cisterns, ready to be released by next action potential • Release of Ca+2 from troponin • Cessation of interaction between actin and myosin
Muscular Contraction • The width of A bands is constant • Z lines move closer
Production of ATP in Muscle Fibers (Tortora & Derrickson, 2006) • 3 ways of ATP production: • From creatine phosphate • Anaerobic cellular respiration (ATP-producing reactions not requiring oxygen) • Aerobic cellular respiration (ATP-producing reactions requiring oxygen, in mitochondria)
Creatine Phosphate • Creatine: small amino acid-like molecule formed in liver, kidneys, pancreas transported to msucles • Relaxed muscles creatine phosphate 3-4x > ATP • Relaxation: ATP + creatine creatine phosphate + ADP (by creatine kinase) • Contraction: creatine phosphate + ADP ATP + creatine (by creatine kinase) • For 15 seconds contraction (100-m dash)
2. Anaerobic Cellular Respiration • Creatine phosphate is depleted then: • Glucose (from blood or from the breakdown of glycogen in muscles) glycolysis 2 pyruvic acid + 2 ATP (produces 4 ATP but net gain of 2 ATP) • Pyruvic acid mitochondria, aerobic respiration ATP • No oxygen (anaerobic) in cytosol: 80% Pyruvic acid lactic acid blood (becomes acid) liver convert back into glucose • For 30 - 40 seconds activity (400-m race)
3. Aerobic Cellular Respiration • Sources of ATP: pyruvic acid, fatty acid (breakdown of triglycerides; yields > 100 ATP), amino acids (breakdown of proteins) • Sufficient oxygen: Pyruvic acid mitochondria oxydized ATP + CO2 + H2O + heat • Slower than glycolysis, but yields 36 ATP • Sources of oxygen: hemoglobin & myoglobin • For > 10 minutes activity (marathon race)
Energy Sources (Ganong, 2005) ATP + H2O ADP + H3PO4 + 7.3 kcal Phosphorylcreatine + ADP ↔ Creatine + ATP Rest & light exercise: FFA CO2 + H2O + ATP Increased intensity of exercise Glucose + 2 ATP (or glycogen + 1 ATP) 2 Lactic acid + 4 ATP (anaerobic) Glucose + 2 ATP (or glycogen + 1 ATP) 6CO2 + 6H2O + 40ATP (aerobic)
100-m dash (10 seconds) 85% of energy is derived anaerobically • 2-mile race (10 minutes) 20% of energy is derived anaerobically • long-distance race (60 minutes) 5% of energy is derived anaerobically
Muscle fatigue: The inability of muscle to maintain force of contraction after prolonged activity, caused by: • Inadequate release of Ca+2 from sarcoplasmic reticulum • Depletion of creatine phosphate • ATP levels = resting levels • Insufficient oxygen • Depletion of glycogen • Buildup of lactic acid & ADP • Failure of action potentials in releasing ACh
Oxygen Consumption after Exercise • Oxygen debt added oxygen, over and above the resting oxygen consumption, taken into the body after exercise • Convert lactic acid glycogen stores in liver (small amount) • Resynthesize creatine phosphate & ATP • Replace the oxygen removed from myoglobin • Much of lactic acid pyruvic acid for ATP production (heart, liver, kidneys, skeletal muscles) • Better term: recovery oxygen uptake ( chemical reactions, heart & muscles still working, recovery processes)
Types of Contraction Isotonic (A) and isometric (B) contraction
Types of Contraction • Isometric (“same length”) contraction: Contraction occurs without an appreciable decrease in the length of the whole muscle do not work (work = force x distance)
Isotonic (“same tension”) contraction: Contraction against a constant load do work
Isotonic contraction Cause more damage
Muscle twitch: brief contraction followed by relaxation of all muscle fibers in a motor unit caused by a single action potential in its motor neuron • “Fast” muscle fibers: fine movements (7.5 ms) • “Slow” muscle fibers: gross movements (100 ms)
Summation of Contractions • No refractory period such as in neuronsin muscle fibers • Repeated stimulation summation of contractions • Tetanus (tetanic contraction) continuous contraction: • Fused (complete) tetanus • Unfused (incomplete) tetanus
Disorders and Abnormalities • Myasthenia gravis: skeletal muscles are weak and tire easily; caused by autoantibodies destroying nicotinic acetylcholine receptors • Lambert-Eaton syndrome: muscle weakness; caused by antibodies against Ca+2 channels in the nerve endings • Denervation hypersensitivity • Contracture: No relaxation due to the inhibition of Ca+2 transport into the reticulum
Disorders and Abnormalities • Hypotonia: decreased or lost muscle tone • Flaccid paralysis loss of muscle tone, loss/ reduction of tendon reflexes, atrophy, degeneration of muscles (disorders of nervous system; electrolytes imbalances (Na+, Ca+2, Mg+2) • Hypertonia: increased muscle tone • Spastic paralysis increased muscle tone, tendon reflexes, pathological reflexes (Babinski sign) • Rigidity increased muscle tone, not reflexes (tetanus)
Disorders and Abnormalities • Muscular dystrophy: progressive weakness of skeletal muscle caused by mutations in genes for muscle proteins • Duchene’s muscular dystrophy dystrophin protein is absent from muscle; X-linked; fatal by 30 y/o • Metabolic myopathies (e.g. McArdle’s syndrome) mutations in genes of enzymes involved in carbohydrates, fats, and proteins, metabolism • Myotonia muscle relaxation is prolonged after contraction; abnormal genes in chromosomes 7, 17, or 19, which produce abnormalities of Na+ or Cl- channels