Download

1 / 1
10 likes | 91 Views
Project Title: Readmission Reduction Date: August 2013 Hospital Name: Henry Mayo Newhall Memorial Medical Center State: California. Run Charts. Aim Statement. Lessons Learned. Add DC Planners . MDT Rounding. SNF/HH communication. EHH Pilot.

E N D
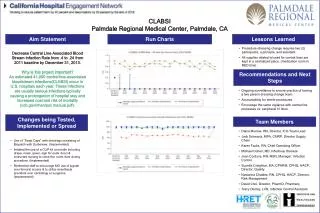
Project Title: Readmission Reduction Date: August 2013 Hospital Name: Henry Mayo Newhall Memorial Medical Center State: California Run Charts Aim Statement Lessons Learned Add DC Planners MDT Rounding SNF/HH communication EHH Pilot Engaging community partners requires someone stepping forward as coordinator/chair. Collaboration with 5 hospitals and 3 home health agencies enhanced the success of the project Establishing communication channels across systems is complex Aim: Reduce hospital readmissions by 20% to 6.6 compared to the 2010 baseline of 8.3 by 12/31/13 Why is this project important? Drill down of readmission data reflected 60% of patients discharged with Home Health (HH) orders that are readmitted within 30 days are actually readmitted in the first 14 days post discharge. Patients being discharged home with home heath were targeted for this project. The project goal is to frontload home health visits within the first 14 days of discharge to reduce readmissions. SFV/SCV Collaborative ED Case Manager Blue Envelope Recommendations and Next Steps First Friday night tuck in call is invaluable in identifying and addressing potential gaps to avoid readmissions. Expand pilot/collaborative to reduce readmission for patient’s discharged to SNF’s Implement follow-up phone calls Changes being Tested, Implemented or Spread Case Management transformation – • Refocus case managers to care coordination (Implemented, Spread). • Established process for concurrent review of ED admissions (Tested, Implemented). • Collaborative Multidisciplinary Team Rounding (Tested, Implemented, Spread ) • Established Santa Clarita Valley / San Fernando Valley community partnerships w/ hospitals, Skilled Nursing Facilities, Home Health agencies (SFV SCV Collaborative) (Implemented). • Blue Discharge Envelopes (Tested, Implemented, Spread). • Adopted Enhanced Home Health project within our community (Tested). • See Flow Chart • Developed effective communication with post-acute providers (Tested, Implemented). Team Members • E Cravitz MSN Case Management Director • C.R. Hudson CFO • Dr Pryor Physician Advisor • A. Nowlin Director of Quality • Case Management and Social Services Staff • T Perez and K Redd Informatics • H. Winkle Access • HSAG partners • Home Health agencies • Hospitals from region