Download
1 / 38
380 likes | 398 Views
Explore a case study of a 47-year-old male experiencing postprandial hypoglycemia after gastric bypass, leading to the discovery of Nesidioblastosis. Learn about diagnosis, differential considerations, and treatment options.

E N D
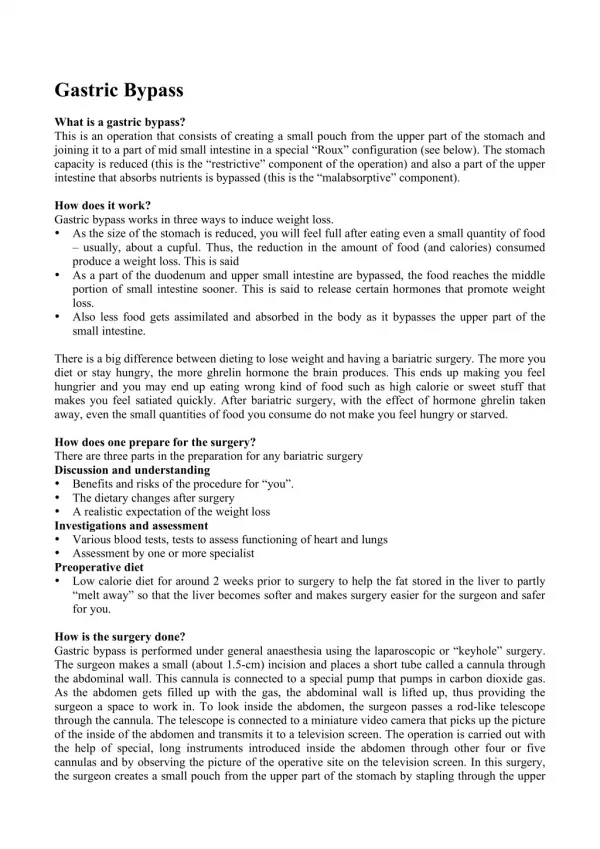
Nesidioblastosis After Gastric-Bypass Surgery Heidi Chamberlain Shea, MD Endocrine Associates of Dallas
Case • 47 year old male presents with recent onset of confusion • Occurs 1-3 hours after meals • Worse with high carbohydrate intake • Resolves when eats or drinks carbohydrates • Blood sugar 53 mg/dl with confusion
Case • History of obesity • Roux-en-Y-gastric bypass 2 years ago • BMI 45 to current 23 • Glucose 53 mg/dl • Insulin 16 µU/ml (< 3) • C-peptide 1.8 ng/ml (< 0.6) • Negative sulfonylurea screen
Non-Beta cell tumors Mesechymal Sarcoma and fibroma Adrenocortical Hepatomas Carcinoid Hormonal deficiencies Cortisol Growth hormone Critical illness Hepatic disease Cardiac disease Renal disease Sepsis Starvation Alimentary (Reactive) Post gastric-bypass Dumping Syndrome Idiopathic Differential DiagnosisHypoglycemia
Differential DiagnosisHypoglycemia • Drugs • Insulin • Sulfonylurea • Alcohol • Pentamidine • Quinine • Salicylates • Sulfonamides
Metabolic disorders Galactosemia Fructose intolerance Fatty acid oxidation defects Glycogen storage disorders Endogenous hyperinsulinism Insulinoma Auto-antibodies to insulin or the β-cell Functional β-cell disorder Differential DiagnosisHypoglycemia
Beta-cell Function SUR 1 (Kir 6.2) α-Ketoglutarate GDH Glutamate
Differential DiagnosisPost-prandial Hypoglycemia • Drugs • Critical illness • Hormonal deficiencies • Non-Beta cell tumors • Endogenous hyperinsulinism • Autoimmune • Metabolic • Alimentary (Reactive)
Case • Does he have an insulinoma? • Should have fasting hypoglycemia • Only occurring after meals is unusual • Imaging • Triple phase spiral CT • Transabdominal ultrasound of the pancreas • Arterial calcium-stimulation testing • Increased insulin from the splenic artery distribution • Underwent partial pancreatectomy
Histology Normal islet Hypertrophic islet cells Insulin cells lining the pancreatic ducts (Nesidioblastosis)
What is Nesidioblastosis? • Pathological description of islet cells budding off pancreatic ducts • Hyperinsulinemic hypoglycemia • Affects the newborn population • Loss of function in Sur 1 (Kir 6.2) • Gain of function GDH and GK • Deletion of chromosome 11p150 • Transient • Diazoxide • Octreotide • Persistent • Partial pancreatectomy
Hyperinsulinemia Hypoglycemia From Gastric-Bypass? Service et. al., NEJM 2005, 353(3):249-54
45 cases in the literature Earliest report 1975 Found due to surgical resection for insulinoma One case after pancreatic transplant No mutations in MEN 1, Sur1 or Kir6.2 Postprandial hypoglycemia Neuroglycopenic symptoms Incidence Male = Female Obese and lean Age 11 to 84 years Hyperinsulinemia Hypoglycemia In Adults?
Questions • Does altering gastric anatomy result in hyperinsulinemia hypoglycemia? • Is weight loss revealing underlying pathology?
Points of Discussion • Discuss the interaction between hormones and regulation of appetite • Review metabolic changes associated with gastric by-pass surgery • Decide if gastric by-pass is a risk factor for hyperinsulinemia hypoglycemia
Appetite Control Wynne et. al., JCEM 2004, 89(6):2576-2582
Ghrelin Secreted from oxyntic cells of stomach Initiates hunger Increases before meal Decreases afterward Increases calorie intake True role in decreasing appetite is debated Intestinal Regulation of Appetite
Peptide YY (PYY) Satiety and nutrient absorption Crosses blood brain barrier Secreted from entire intestine Greater in distal L cells Stimulated by food via vagal stimulation Increased levels High calorie Fat Inactivated by dipeptidyl peptidase IV (DPPIV) Pancreatic polypeptide (PP) Satiety and nutrient absorption Produced by pancreas Colon and rectum Stimulated by food More is released with later meals of the day Increased with anorexia Variable levels seen with obesity Intestinal Regulation of Appetite
Intestinal Regulation of Appetite Wynne et. al., JCEM 2004, 89(6):2576-2582
Glucagon-like peptides (GLP-1 & 2) Satiety Expressed in brain, pancreas and small intestine L-cells Stimulated by food Acts via the GLP-1 receptor Augments postprandial insulin secretion Decreases gastric motility Inhibits gastric acid secretion Oxyntomodulin (OXM) Satiety Expressed in brain, and small intestine L-cells Stimulated by food Acts via the GLP-1 receptor Augments postprandial insulin secretion Decreases gastric motility Inhibits gastric acid secretion Meal termination Inhibits Ghrelin Intestinal Regulation of Appetite
Intestinal Regulation of Appetite • Cholecystokinin (CCK) • Satiety and nutrient absorption • Released by duodenum and jejunum • L cells • Stimulated by intraluminal food
Bariatric Surgery Gastric Banding 30-50% weight loss Roux-en-Y-gastric bypass 50-80% weight loss
Bariatric Surgery • Most effective way to achieve weight loss • Reduces weight by 35-40% • Maintained for 15 years • Decreases appetite • Malabsorption is limited
Immediate post surgical risks Malabsorption Limited time Dumping syndrome Nausea Bloating Colic Diarrhea Light headedness Diaphoresis Palpitations Bariatric SurgeryComplications
Improves obesity-related comorbidities Diabetes Hypertension Dyslipidemia Nonalcoholic steatosis Sleep apnea Reflux esophagitis Venous stasis ulcers Infertility Arthritis Pseudotumor cerebri Stress incontinence Bariatric SurgeryBenefits
Bariatric SurgeryPhysiology Banded N=17 Control N=17 Dixon et al., JCEM 2005, 90(2):813-19
Bariatric SurgeryPhysiology Glucose mg/dl Insulin uIU/L 60 135 50 125 40 115 30 105 20 95 10 85 0700 0900 1000 1100 0700 0900 1000 1100 □ BMI matched controls N=17 ●○ Lap band patients N=17 Dixon et al., JCEM 2005, 90(2):813-19
Gastric-bypassHormonal Changes • After bypass • Ghrelin variable results • Leptin decreases • Glucose decreases • Insulin decreases • Adiponectin increases • CCK, VIP and Serotonin unaffected
Gastric-bypassHormonal Changes • Future studies • Response of other intestinal hormones • Understand the complex interactions between hormones and appetite • Other unidentified players?
Hyperinsulinemia Hypoglycemia From Gastric-Bypass? Service et. al., NEJM 2005, 353(3):249-54
β-cell Proliferation • Authors postulate that gastric-bypass increases incretin like substances • Increased bolus delivery to distal small intestine • β-cells stimulated to increased insulin secretion = hypertrophy • What happens to islet cells with incretin supplementation?
Animal StudiesExenatide • Non diabetic obese male Zucker rats • 3 groups • Control given saline • N=11 • Exenatide treated and PO ad lib • N=10 • Pair fed • N=10 • 6 week study Gedulin, B. R. et al. Endocrinology 2005;146:2069-2076
Animal StudiesExenatide Gedulin, B. R. et al. Endocrinology 2005;146:2069-2076
Animal StudiesExenatide ● Ex ∆ PF ○ CL • Absolute mass unchanged • No comment about hypertrophy • Absolute β-cell mass • Improved sensitivity • Decrease in β-cell mass • No evidence for hypertrophy in presence of incretins Gedulin, B. R. et al. Endocrinology 2005;146:2069-2076
Conclusions • Does altering gastric anatomy result in hyperinsulinemia hypoglycemia? • Currently no evidence to support • Is weight loss revealing underlying pathology? • Possibly • Insulin resistance is protective • Patients that need surgery • Unknown defect in β-cell function
Hypoglycemia TrialsAre patients not identified? • Multiple studies • Patients are rarely hypoglycemic with symptoms • Normal non-symptomatic patient can be hypoglycemia • Brun JF, et. al., Diabetologia 1995, 38(4) • Palardy J et. al., NEJM 1989, 321(21) • Buss RW et. al., Hormone & Metabolism Research 1982, 14(6) • Lev-Rau et al, Diabetes 1981, 30(12)