Download
1 / 1
10 likes | 100 Views
Comparison of susceptibility testing methods for determining Ceftazidime resistance in Pseudomonas aeruginosa. D-735/178 50 th ICAAC Sept. 12-15, 2010 Boston. V. E. DANIEL, M. WOOTTON, R.A. HOWE. Methods

E N D
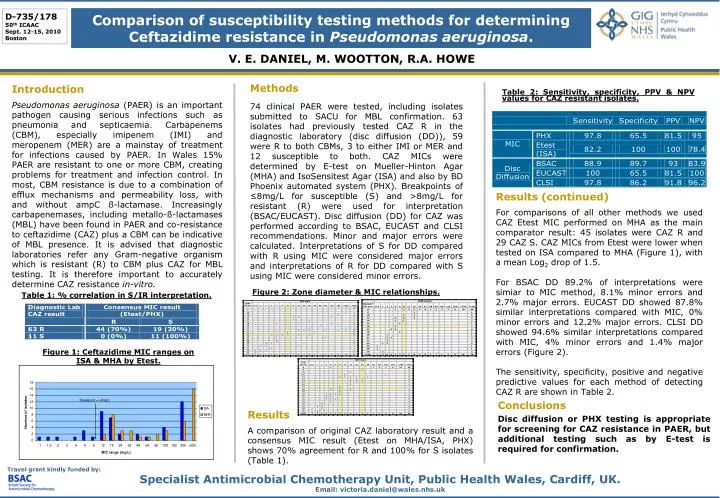
Comparison of susceptibility testing methods for determining Ceftazidime resistance in Pseudomonas aeruginosa. D-735/178 50th ICAAC Sept. 12-15, 2010 Boston V. E. DANIEL, M. WOOTTON, R.A. HOWE Methods 74 clinical PAER were tested, including isolates submitted to SACU for MBL confirmation. 63 isolates had previously tested CAZ R in the diagnostic laboratory (disc diffusion (DD)), 59 were R to both CBMs, 3 to either IMI or MER and 12 susceptible to both. CAZ MICs were determined by E-test on Mueller-Hinton Agar (MHA) and IsoSensitest Agar (ISA) and also by BD Phoenix automated system (PHX). Breakpoints of ≤8mg/L for susceptible (S) and >8mg/L for resistant (R) were used for interpretation (BSAC/EUCAST). Disc diffusion (DD) for CAZ was performed according to BSAC, EUCAST and CLSI recommendations. Minor and major errors were calculated. Interpretations of S for DD compared with R using MIC were considered major errors and interpretations of R for DD compared with S using MIC were considered minor errors. Introduction Pseudomonas aeruginosa (PAER) is an important pathogen causing serious infections such as pneumonia and septicaemia. Carbapenems (CBM), especially imipenem (IMI) and meropenem (MER) are a mainstay of treatment for infections caused by PAER. In Wales 15% PAER are resistant to one or more CBM, creating problems for treatment and infection control. In most, CBM resistance is due to a combination of efflux mechanisms and permeability loss, with and without ampC ß-lactamase. Increasingly carbapenemases, including metallo-ß-lactamases (MBL) have been found in PAER and co-resistance to ceftazidime (CAZ) plus a CBM can be indicative of MBL presence. It is advised that diagnostic laboratories refer any Gram-negative organism which is resistant (R) to CBM plus CAZ for MBL testing. It is therefore important to accurately determine CAZ resistance in-vitro. Table 2: Sensitivity, specificity, PPV & NPV values for CAZ resistant isolates. Results (continued) For comparisons of all other methods we used CAZ Etest MIC performed on MHA as the main comparator result: 45 isolates were CAZ R and 29 CAZ S. CAZ MICs from Etest were lower when tested on ISA compared to MHA (Figure 1), with a mean Log2 drop of 1.5. For BSAC DD 89.2% of interpretations were simiar to MIC method, 8.1% minor errors and 2.7% major errors. EUCAST DD showed 87.8% similar interpretations compared with MIC, 0% minor errors and 12.2% major errors. CLSI DD showed 94.6% similar interpretations compared with MIC, 4% minor errors and 1.4% major errors (Figure 2). The sensitivity, specificity, positive and negative predictive values for each method of detecting CAZ R are shown in Table 2. Figure 2: Zone diameter & MIC relationships. Table 1: % correlation in S/IR interpretation. Figure 1: Ceftazidime MIC ranges on ISA & MHA by Etest. Conclusions Disc diffusion or PHX testing is appropriate for screening for CAZ resistance in PAER, but additional testing such as by E-test is required for confirmation. Results A comparison of original CAZ laboratory result and a consensus MIC result (Etest on MHA/ISA, PHX) shows 70% agreement for R and 100% for S isolates (Table 1). Travel grant kindly funded by: Specialist Antimicrobial Chemotherapy Unit, Public Health Wales, Cardiff, UK. Email: victoria.daniel@wales.nhs.uk