Download
1 / 21
290 likes | 982 Views
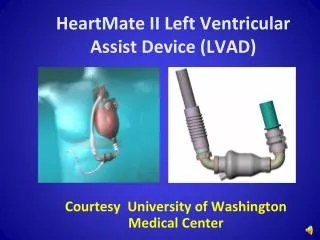
Post Operative Care of the Left Ventricular Assist Device Patient in the Acute Care Setting. Presented by Jude Melendez, MS, RN, CCRN- CSC and Loretta Nerney, BS, RN, CCRN. Key Concepts. T he newly implanted LVAD patient is a post op cardiac surgery patient first, LVAD patient second.

E N D
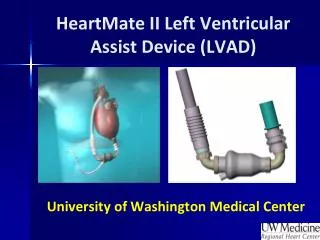
Post Operative Care of the Left Ventricular Assist Device Patient in the Acute Care Setting Presented by Jude Melendez, MS, RN, CCRN- CSC and Loretta Nerney, BS, RN, CCRN
Key Concepts • The newly implanted LVAD patient is a post op cardiac surgery patient first, LVAD patient second. • Nurses need a good understanding of LVAD pump physiology for hemodynamic monitoring.
Goal of LVAD therapy: • Increase CO • Improve end-organ function • Improve Quality of Life • Improve morbidity and mortality Reprinted with the permission of Thoratec Corporation
Pump Physiology • Continuous-flow LVADs deliver flow throughout the entire cardiac cycle • Flow is determined by • Pump speed: Flow increases with speed increases • Preload dependent • Afterload sensitive • The aortic valve may not always open and patients may not have a palpable pulse
Pulsatility Index (PI) • As the left ventricle contracts and relaxes, the flow through the pump increases and decreases, adding a degree of pulsatility • PI is the magnitude of this flow pulse • The pulsatility index (PI) will normally decrease as pump speed is increased • PI will change with patient conditions that normally affect stroke volume (physiologic demand, volume status, RV function)
Suction Events If pump speed is set too high or conditions exist to affect preload, the pump may decompress the LV to the point of collapsing the walls together. Evaluate the cause – they are the same complications that can arise for any cardiac surgery patient • Hypovolemia/vasodilation (affecting preload) • Post-operative bleeding • Tamponade • Arrhythmia • RV failure Reprinted with the permission of Thoratec Corporation
Nursing Assessments Systems Survey Device Parameters and Hemodynamics Monitoring for complications Patient and Caregiver needs
Hemodynamic Assessments • Arterial line • Swan-Ganz catheter • Physical S/S of good perfusion • TEE when in doubt
Device Parameters Monitor for variations from patient baseline
Arterial waveform for LVAD patients http://pics3.this-pic.com/key/dampened%20arterial%20line%20waveform
Systems Survey: Cardiac Therapy Goals & Interventions • MAP 70-85 mmHg • Normothermia • Pressors (dopamine, vasopressin, levophed) • Fluid resuscitation • Cardiac Index > 2.2, LVAD flow > 3.5 liters/minute • Adequate preload • Balance RV failure vs. adequate LVAD filling • Increase RV contractility (epi, primacor) • Decrease RV afterload: iNO • Treat arrhythmias promptly – protect heart function • Monitor labs: abg, mvg, lactic acid
Systems Survey • Neuro status • Pain management and sedation • Evaluate for CVA • Pulmonary status • If on iNO, ventilator dependent until weaned off • SaO2 may not be obtainable; correlate to abg • Underlying pulmonary dysfunction • Hematologic status • Assess for bleeding: chest tubes, incisions, drive line site • Monitor H/H, TEG, Coags • Hemolysis? Monitor LDH
Systems Survey • Renal function: assess for adequate perfusion& functioning • Monitor/replace electrolytes • Monitor urine output • Monitor BUN/creatinine • Hepatic function: assess for dysfunction from pre-op history of heart failure • Assess for coagulopathies • Blood glucose control
Systems Survey • Infection control • Antibiotic prophylaxis • Address all risk factors: nutrition, mobility& skin integrity, glucose control, sterile dressing changes, drive line protection • GI function & Nutrition • Promote gastrointestinal motility post op • Assess pre-albumin levels
RED HEART ALARM Rule out power failure or equipment malfunction. Otherwise, there is a low pump flow state. Assess the patient for post-op complications. Reprinted with the permission of Thoratec Corporation
Complications: LOW FLOW Low Flow and Low CVP • Replace volume • Give vasoconstrictors if right heart is weak • Check H/H; rule out bleeding • Rule out mechanical versus coagulopathy • Monitor H/H, platelet, PT, PTT, Fibrinogen, TEG : replace products, administer protamine • Monitor chest tube drainage
Complications: LOW FLOW High CVP & suction events • RV Failure • Possible Causes : Any increase in RV afterload; pulmonary HTN, volume overload, acidosis, hypoxia, ischemia, pulmonary embolus • Cardiac Tamponade • S/S: Hypotension, elevated filling pressures, reduced SvO2, reduced urine output, slowed chest tube output • CXR/CT scan
Complications: LOW FLOW Other Low Flow Considerations • Pump thrombus • may see power spikes, grating or rough pump noise, falsely high pump flows, clinical signs of heart failure, increased native pulsatility, hemolysis • Treatment: anticoagulant or thrombolytic therapy, possible pump exchange • Arrhythmia • NO CHEST COMPRESSIONS/ OK TO DEFIBRILLATE • Inflow cannula obstruction (septal occlusion) • may see reduced pump speed and hear device chatter • High afterload • Rx with vasodilators
Safety Pearls • No chest compressions • ACLS drugs and cardiac defibrillation OK to give • No MRI • Avoid getting system components wet • Maintain patient equipment and keep a spare system controller and a spare power source with the patient at all times
Transitioning care Psychosocial needs Educational needs Elements for discharge to home VAD support group
References O’Shea, G. (2012). Ventricular Assist Devices: What Intensive Care Unit Nurses Need to Know About Postoperative Management. AACN Advanced Critical Care. 23(1) 69-83. Slaughter, M., Pagani, F., Rogers, J., Miller, L., Sun, B., Russell, S. …Farrar, D.(2010). Clinical Management of Continuous-flow Left Ventricular Assist Devices in Advanced Heart Failure. The Journal of Heart and Lung Transplantation. 29(4S) S1-S39. Thoratec Corporation. (2012). HeartMate II Left Ventricular Assist System LVAS: Instructions for Use. Pleasanton, CA: Thoratec Corporation.