Download
1 / 86
860 likes | 1.02k Views
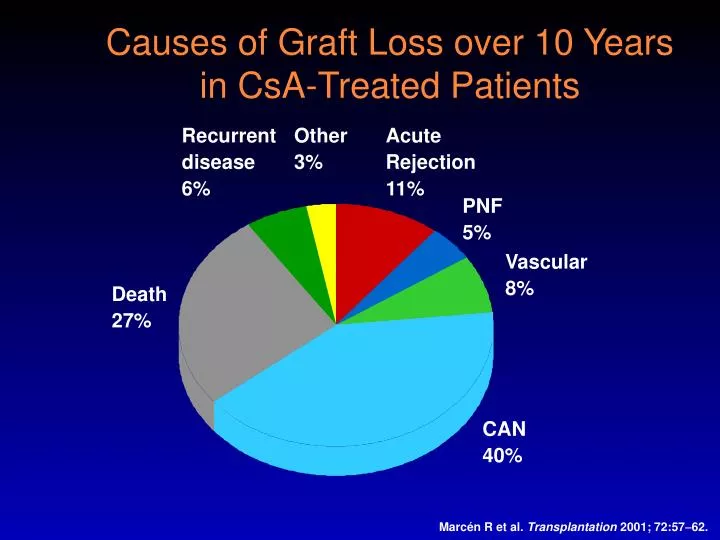
Causes of Graft Loss over 10 Years in CsA-Treated Patients. Recurrent disease 6% . Other 3%. Acute Rejection 11% . PNF 5%. Vascular 8%. Death 27%. CAN 40%. Marcén R et al. Transplantation 2001; 72:57 62. Presentation techniques Some personal advice. I. Performance

E N D
Causes of Graft Loss over 10 Years in CsA-Treated Patients Recurrent disease 6% Other 3% Acute Rejection 11% PNF 5% Vascular 8% Death 27% CAN 40% Marcén R et al. Transplantation 2001; 72:5762.
Presentation techniquesSome personal advice • I. Performance • II. Manuscript • III. Slides
Presentation techniquesSome personal advice • I. Performance • II. Manuscript • III. Slides
I. Performance • Never turn your back on the audience • Always look at the audience • (and the laptop)
I. Performance • Never turn your back on the audience • Always look at the audience • (and the laptop) • Never use the laser pointer • Always use your slides to make your point
Causes of Graft Loss over 10 Years in CsA-Treated Patients Recurrent disease 6% Other 3% Acute Rejection 11% PNF 5% Vascular 8% Death 27% CAN 40% Marcén R et al. Transplantation 2001; 72:5762.
Causes of Graft Loss over 10 Years in CsA-Treated Patients Recurrent disease 6% Other 3% Acute Rejection 11% PNF 5% Vascular 8% Death 27% CVD CNI- nephrotox CAN 40% Marcén R et al. Transplantation 2001; 72:57-62.
Metabolic Toxicities of Immunosuppressive Drugs CsA = cyclosporine A; Tac = tacrolimus; Ster = corticosteroids; SRL/EVL = sirolimus/everolimus; AZA = azathioprine Adapted from Danovitch GM. Transplant Rev 2000; 14:65–81.
Metabolic Toxicities of Immunosuppressive Drugs CsA = cyclosporine A; Tac = tacrolimus; Ster = corticosteroids; SRL/EVL = sirolimus/everolimus; AZA = azathioprine Adapted from Danovitch GM. Transplant Rev 2000; 14:65–81.
Metabolic Toxicities of Immunosuppressive Drugs CsA = cyclosporine A; Tac = tacrolimus; Ster = corticosteroids; SRL/EVL = sirolimus/everolimus; AZA = azathioprine Adapted from Danovitch GM. Transplant Rev 2000; 14:65–81.
Metabolic Toxicities of Immunosuppressive Drugs CsA = cyclosporine A; Tac = tacrolimus; Ster = corticosteroids; SRL/EVL = sirolimus/everolimus; AZA = azathioprine Adapted from Danovitch GM. Transplant Rev 2000; 14:65–81.
Metabolic Toxicities of Immunosuppressive Drugs CsA = cyclosporine A; Tac = tacrolimus; Ster = corticosteroids; SRL/EVL = sirolimus/everolimus; AZA = azathioprine Adapted from Danovitch GM. Transplant Rev 2000; 14:65–81.
0.6 0.5 0.4 0.3 0.2 0.1 0 400 0 50 100 150 200 250 300 350 450 500 Daclizumab Reduces the Risk of Biopsy-Proven Acute Rejection (BPAR) • Cumulative incidence of first BPAR • Pooled analysis of 12-month data from two pivotal trials Placebo (n=268) 116 events Daclizumab (n=267) 74 events Probability p = 0.0001 (stratified logrank test) Time after transplantation (days) Ekberg H et al. Transplant Int 2000; 13:151–9.
0.6 0.5 0.4 0.3 0.2 0.1 0 400 0 50 100 150 200 250 300 350 450 500 Daclizumab Reduces the Risk of Biopsy-Proven Acute Rejection (BPAR) • Cumulative incidence of first BPAR • Pooled analysis of 12-month data from two pivotal trials Placebo (n=268) 116 events Daclizumab (n=267) 74 events Probability p = 0.0001 (stratified logrank test) Time after transplantation (days) Ekberg H et al. Transplant Int 2000; 13:151–9.
I. Performance • Never turn your back on the audience • Always look at the audience • Never use the laser pointer • Always use your slides to make your point • Always time your performance at home • 3 - 7 - 10 - 20 minutes sharp
I. Performance • Never turn your back on the audience • Always look at the audience • Never use the laser pointer • Always use your slides to make your point • Always time your performance at home • Always prepare your opening sentences
Opening sentence You will always be nervous: Sit in the front - look back Prepare your opening sentence - the rest will come by itself
Opening sentence You will always be nervous: Sit in the front - look back Prepare your opening sentence - the rest will come by itself Mr chairman, ladies and gentlemen! (.) For many years (.) steroids have been the backbone (.) of our manitenance IS (.) Now is the time to challenge them (.)
Opening sentence You will always be nervous: Sit in the front - look back Prepare your opening sentence - the rest will come by itself Members and guests (.) I thank the organizers for inviting me (.) and I thank all of you for joining us (.) in this symposium tonight (.) Do not repeat the title of your talk
Presentation techniquesSome personal advice • I. Performance • II. Manuscript • III. Slides
II. Manuscript • Never read a manuscript of your talk • Always use your slides as the manuscript
150-300 ng/ml for 3 months 100-200 ng/ml thereafter A Normal dose CsA MMF Steroids 50–100 ng/ml Daclizumab Low dose CsA B MMF Steroids 3-7 ng/ml Daclizumab Low dose TAC C MMF Steroids 4-8 ng/ml Daclizumab Low dose SRL D MMF Steroids SYMPHONY Study Design 6 mo 12 mo Tx Ekberg H et al Am J Transpl 2006, 6 (suppl 2), #49; 83.
Symphony study Main inclusion criteria • Renal transplant recipients 18 75 years • Single-organ, kidney • Living or deceased donors Main exclusion criteria • Panel reactive antibodies > 20% • Cold ischaemic time > 30 hours • History of malignancy
Never read a manuscript • Always use your slides as the manuscript • Always describe your slide immediately II. Manuscript
p=0.0014 p<0.0001 p<0.0001 Calculated GFR(CockcroftGault) 100 90 80 Normal-dose CsA 65 70 59 Low-dose CsA 57 57 60 Low-dose TAC GFR (Cockcroft Gault) (ml/min) 50 Low-dose SRL 40 30 20 10 0 12 months post-Tx Ekberg H et al Am J Transpl 2006, 6 (suppl 2), #49; 83.
High Prevalence of Subclinical Rejection (SCR) • Prevalence SCR • 1 mo 61 % • 3 mo 46 % • 1 yr 26 % 80 60 Prevalence (%) 40 Acute rejection SCR (acute) 20 SCR (borderline) 0 10 0.1 0.25 0.5 1 2 3 4 5 6 7 8 9 Time after transplantation (years) Nankivell BJ et al. N Engl J Med 2003; 349:232633.
II. Manuscript • Never read a manuscript • Always use your slides as the manuscript • Always describe your slide immediately • Never start with comments
II. Manuscript • Never read a manuscript • Always use your slides as the manuscript • Always describe your slide immediately • Never start with comments • let comments come last • make one extra slide
p=0.0014 p<0.0001 p<0.0001 Calculated GFR(CockcroftGault) 100 90 80 Normal-dose CsA 65 70 59 Low-dose CsA 57 57 60 Low-dose TAC GFR (CockcroftGault) (ml/min) 50 Low-dose SRL 40 30 No significant difference between CsA and Low-CsA 20 10 0 12 months post-Tx Ekberg H et al Am J Transpl 2006, 6 (suppl 2), #49; 83.
High Prevalence of Subclinical Rejection (SCR) • Prevalence SCR • 1 mo 61 % • 3 mo 46 % • 1 yr 26 % 80 60 Prevalence (%) 40 Acute rejection SCR (acute) 20 SCR (borderline) 0 10 0.1 0.25 0.5 1 2 3 4 5 6 7 8 9 Time after transplantation (years) Nankivell BJ et al. N Engl J Med 2003; 349:232633.
High Prevalence of Subclinical Rejection (SCR) • Prevalence SCR • 1 mo 61 % • 3 mo 46 % • 1 yr 26 % 80 High risk for AR after CNI w/d Lower risk 60 Prevalence (%) 40 Acute rejection SCR (acute) 20 SCR (borderline) 0 10 0.1 0.25 0.5 1 2 3 4 5 6 7 8 9 Time after transplantation (years) Nankivell BJ et al. N Engl J Med 2003; 349:2326-33.
II. Manuscript • Never read a manuscript • Always use your slides as the manuscript • Always describe your slide immediately Why is this so important? Because the audience cannot read your slide and listento you at the same time - > Competition
II. Manuscript • Never read a manuscript • Always use your slides as the manuscript • Always describe your slide immediately - > Competition TV news + kids TV news + Radio news
II. Manuscript • Never read a manuscript • Always use your slides as the manuscript • Always describe your slide immediately • Always send on one channel at the time So read your text with them first then give your comments TV news first, then radio
Methods • Acute rejection was defined as biopsy-proven and treated events within 6 months after transplantation excluding borderline cases
Methods • Acute Rejection • Biopsy-proven • Treated patients • Within 6 mo. • Excluding Borderline
II. Manuscript • Never read a manuscript • Always use your slides as the manuscript • Always describe your slide immediately • Send on one channel at the time • Always use a strategy • (chapters, line of thoughts)
Strategy This is a study that shows the benefit of steroid withdrawal … the study… In conclusion, this study has shown the benefit of steroid withdrawal. • First, say what you are going to tell us • Then tell us • Finally, say what you have told us
Chapters • Divide your talk into chapters • 1. Background • 2. Aim • 3. Method • 4. Results • 5. Conclusion
Chapters • Divide your talk into chapters • 1. Background - 2 slides • 2. Aim - 1 slide • 3. Method - 2 slides • 4. Results - 3 slides • 5. Conclusion - 1 slide • 8 - 10 slides = 7 minutes
Presentation techniquesSome personal advice • I. Performance • II. Manuscript • III. Slides
III. Slides • Never apologize for a busy slide • - discard it! • Never say ’as you can see’ • it means nobody can see!
Table 2. Multivariate Risk Estimates for Endpoint of Overall Graft Loss* This is actually a slide that was used in a congress *Table displays main variable of interest and significant (α < .05) covariates in the model.
Multivariate risk estimates for graft loss Somebody et al ATC 2004
Multivariate risk estimates for graft loss Somebody et al ATC 2004
Multivariate risk estimates for graft loss Somebody et al ATC 2004
Multivariate risk estimates for graft loss Somebody et al ATC 2004
Multivariate risk estimates for graft loss Somebody et al ATC 2004
Creatinine levels in posttransplant periods by CNI Kaplan and Meier-Kriesche ATC 2004
Creatinine levels in posttransplant periods by CNI Kaplan and Meier-Kriesche ATC 2004