Download
1 / 20
200 likes | 289 Views
Day for Night: Hospital Admissions for Day Surgery Patients in California, 2005. Mary Tran, PhD, MPH Healthcare Outcomes Center OSHPD Brian Paciotti, PhD Healthcare Outcomes Center OSHPD Geeta Mahendra University of California, Davis Dept. of Internal Medicine. Presenter Disclosures.

E N D
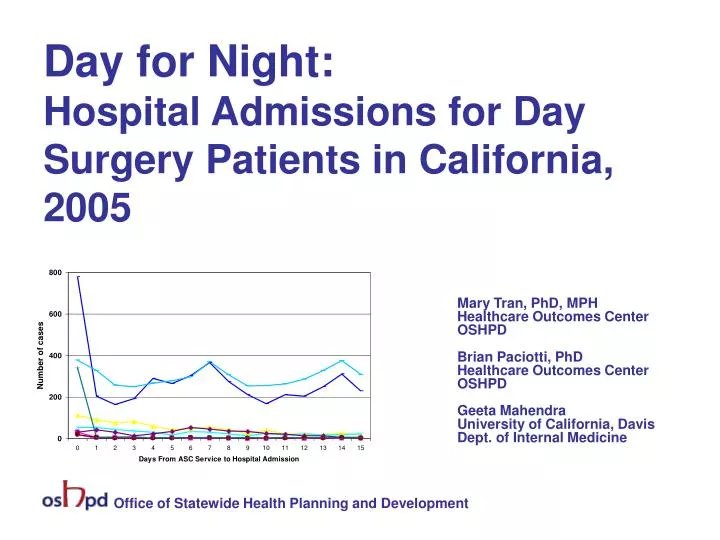
Day for Night: Hospital Admissions for Day Surgery Patients in California, 2005 Mary Tran, PhD, MPH Healthcare Outcomes Center OSHPD Brian Paciotti, PhD Healthcare Outcomes Center OSHPD Geeta Mahendra University of California, Davis Dept. of Internal Medicine Office of Statewide Health Planning and Development
Presenter Disclosures Mary Nelson Tran, PhD, MPH (1) The following personal financial relationships with commercial interests relevant to this presentation existed during the past 12 months: “No relationships to disclose” Office of Statewide Health Planning and Development
Background • Increasing volume of surgical procedures performed in Ambulatory Surgery Centers (ASCs) since 1980s. • Related to improvements in medical technologies and rising cost of inpatient care. • Concerns of providers and public about safety of outpatient procedures. • Objectives of this study • Characterize the pattern of post-ASC admissions to the hospital • Identify risk factors for post-ASC admission • Compare mortality rates for hospital vs. ASC surgery patients receiving comparable procedures. Office of Statewide Health Planning and Development
Methods Data Sources: • Inpatient admissions: Patient Discharge Data (PDD), 2005 • ASC patient encounters: Ambulatory Surgery Data (AS), 2005 • Submitted by California-licensed ASCs (2005 = 1st year of data) • Free-standing surgery clinics, hospital-associated surgery centers • Death during 2005 • California Vital Statistics, Death Statistical Master File, 2005 Linkage: • Linked by Social Security Number, using LinkPlus Analysis (SAS, ver. 9.1): • Logistic regression: • Risk of post-ASC hospital admission • Comparing patients of free-standing vs. hospital-associated ASCs • Risk of death • Comparing surgical patients of hospitals vs. ASCs • Controlling for demographics, severity, payer. Office of Statewide Health Planning and Development
Measures and Definitions • Death • Death Certificate date of death 0-30 days after ASC procedure • Inpatient Admission • First inpatient admission 0-15 days after ASC service date • Diagnoses • ICD-9, principal diagnosis • Coded by Clinical Classifications Software (CCS), AHRQ* • Procedures • Inpatients: Principal procedure, ICD-9 procedure code (CCS categories) • ASC Cases: Principal procedure, CPT code (CCS categories) • Selected Procedures: Surgical** and diagnostic procedures*** frequently performed in both ASC and hospital settings • Patient Acuity (severity of illness) • Charlson Co-morbidity Index, based on ICD-9 diagnosis codes (range 0-17) *Clinical Classifications Software, Agency for Healthcare Quality and Research (AHRQ). http://www.hcup-us.ahrq.gov/toolssoftware/cc/ccs.jsp. ** A Russo, P Owens, C Steiner, J Josephsen. Ambulatory Surgery in U.S. Hospitals, 2003. HCUP Fact Book No. 9. (Healthcare Cost and Utilization Project). http://ahrq.gov/data/hcup/factbk9. *** Two diagnostic procedures frequently performed in both settings in California. Analyses by author. Office of Statewide Health Planning and Development
Volume of ASC Cases and post-ASC Hospital Admissions Total ASC encounters = 2,552,177 • Cases with post-ASC hospital admission within 15 days = 57,678 (2.3%) Of these post-ASC admissions to the hospital: • Route of admission • Emergency Department = 40.1% • Reported source of admission • Home = 89.8% • Ambulatory Surgery = 2.7% • Other inpatient care = 5.2% • SNF, residential care = 2.1% • Other = 0.2% • Time from ASC service to inpatient admission: • 0 to 1 Days = 14.2% • 2 to 7 Days = 38.1% • 8 to 15 Days = 47.6% Office of Statewide Health Planning and Development
Top 10 Hospital Diagnoses for post-ASC Hospital Admissions Office of Statewide Health Planning and Development
Risk factors for post-ASC admission to hospital within 15 days Office of Statewide Health Planning and Development
For cases with post-ASC admission: ASC procedures with highest 30-day mortality Office of Statewide Health Planning and Development
Volume of Selected Procedures* Performed in ASCs and Hospitals * HCUP Fact Book No. 9: Ambulatory Surgery in U.S. Hospitals, 2003, Surgical procedures commonly performed in both inpatient and outpatient settings; plus additional procedures frequently performed in both settings in California (PTCA, cardiac catheterization), author’s analysis. Office of Statewide Health Planning and Development
Characteristics of Patients Receiving the Selected Procedures Office of Statewide Health Planning and Development
Risk of 30-Day Mortality for Selected Procedures Office of Statewide Health Planning and Development
Limitations • Possible bias introduced by exclusion of records with unusable SSNs. • Relied on principal diagnosis and principal procedure only. Secondary dx and tx information might be important. • The Charlson Co-morbidity Index Total Score might not be sufficient to adjust for differences in patient acuity between hospital inpatients and ASC patients. • Only state-licensed ambulatory care facilities submitted data to OSHPD. These results may not reflect admission and mortality risk for procedures performed in other types of outpatient settings. • Due to 2007 court decision, free-standing ASCs are not required to be licensed by the State of California. As a result, they are no longer required to submit patient data to OSHPD. As of October 2008, only 25 (19.7%) of the 127 free-standing ASCs have decided to continue reporting patient data to OSHPD. Office of Statewide Health Planning and Development
Summary and Conclusions • Post-ASC admission within 15 days: • Most come to the hospital from home and 2 out of 5 enter via the Emergency Department. • Half occur a week or more after the ASC service • Likelihood greater if patients have co-morbidities or get care in a hospital-associated facility. • Most frequent diagnosis: Complication of [prior] surgical procedure or medical care. • Inpatient vs. Outpatient Mortality • Risk of death may be higher for ASC patients for some procedures. • Risk of death is greater for patients who have co-morbidities or pay for care out-of-pocket. • Only a small percentage of post-ASC admissions are identified in hospital discharge records. Office of Statewide Health Planning and Development
Acknowledgements • Geeta Mahendra: LinkPlus linkages • Brian Paciotti, PhD: Linkage, coding for CCS and Charlson Co-morbidity Index, SAS analyses • Niya Fong: SAS analyses Office of Statewide Health Planning and Development
Questions and comments Office of Statewide Health Planning and Development
Backup slides Office of Statewide Health Planning and Development
Charlson Co-morbidity Index Components Office of Statewide Health Planning and Development
Days from procedure to inpatient admission, for selected ASC procedures Note: Of all inpatient readmissions within 15 days, 14% occurred in 0-1 days. Of all admissions, 1,551 (2.7%) were coded in PDD as admissions from an ASC. Office of Statewide Health Planning and Development
Days from procedure to inpatient admission, for selected ASC procedures: expanded lower range Office of Statewide Health Planning and Development