Download
1 / 10
100 likes | 223 Views
Resolution of Discordant Confirmatory Results on POC Reactive Rapid Tests: Florida’s Pilot Project. HIV Diagnostics: New Developments and Challenges Feb. 28, 2005 Berry Bennett, MPH Retrovirology Section Chief FL. Bureau of Laboratories Jacksonville, FL.

E N D
Resolution of Discordant Confirmatory Results on POC Reactive Rapid Tests: Florida’s Pilot Project HIV Diagnostics: New Developments and ChallengesFeb. 28, 2005 Berry Bennett, MPHRetrovirology Section ChiefFL. Bureau of LaboratoriesJacksonville, FL.
Public Health Laboratories (PHL) Role in Rapid HIV Testing Provide Confirmation testing on POC presumptive positive rapid tests. Provide quality assurance testing on POC negatives, if applicable? Participate in site specific QA programs- provide technical training needs - provide blood borne pathogen and biohazard safety training - provide proficiency samples and/or encourage CDC’s MPEP enrollment. - provide competency evaluations (site visits?) - provide verification samples and/or quality controls more?? (regulatory consults, troubleshooting, etc.)In July/August 2004 the Association of Public Health Laboratories (APHL) conducted a survey of 56 state and territorial PHLs to assess HIV diagnostic testing practices. The survey included questions as to utilization of rapid tests within PHLs and the roles that PHLs have played in training for non-traditional testing facilities. - Approximately 10% of the respondents indicated use of rapid tests (in-house algorithm vs. study related vs. off-site PHL supported, not specified). - 45% of PHLs have delivered at least one rapid HIV training course, either their own design or CDC.
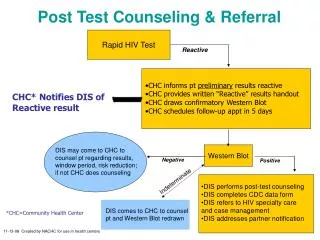
Confirmation Algorithm* for HIV Rapid Testing POC presumptive positive rapid testHIV-1 Western blot or IFA (serum, plasma, dbs)(Orasure W.Blot only)Positive Negative Indeterminate Report as Report as Report asHIV-1 Positive HIV-1 Negative, HIV-1 Indeterminate, request blood (blood) advise 30 day retest. follow up, (Orasure) request blood retest. *CDC Guidelines for a Quality Assurance Program,March, 31, 2003. www.cdc.gov/hiv/rapid_testing
Florida Confirmation Algorithm for HIV Rapid Testing POC presumptive positive rapid test HIV-1 Western blot HIV-1/2 Plus O EIA (serum, plasma, dbs, Orasure) HIV-1 Orasure EIA (comparative purposes)Positive Negative IndeterminateReport as HIV-2 testing (serum, plasma)HIV-1 Positive OraQuick retesting (serum, plasma) Unigold HIV-1 (comparative purposes)possible STARHS case (serum, plasma) (except Orasure)
Expectations in the Confirmation of POC Presumptive Positive Rapid Tests? Provide quick TAT (county jails, drug treatment centers, ERs) Adjust traditional testing algorithms to accommodate a quick TAT Serum, plasma or dbs are preferred specimens however Orasure may be the only alternative for some sites. Provide additional testing (NAAT, Ag+, etc) or refer to CDC to resolve discordance between rapid and traditional laboratory results.
Florida Department of HealthOraQuick Pilot Study(Summer 2003 – Dec. 2004) POC tests performed = 27,473POC negative results = 26,695POC “presumptive positives” = 778Lab-confirmed positives = 764 (98%)Initial rapid tests non-confirmed‡ = 14*Seropositivity rate = 2.78%‡Western Blot negative or indeterminate.*(7) confirmation specimen submitted was unsatisfactory for rapid retesting. (4) OraQuick negative upon repeat (possible POC user misinterpreted) (3) OraQuick positive upon repeat (assay false positive)
Discordant Review of POC Presumptive Positive OraQuicks:Florida, Summer 2003 – 12/31/2004 Confirmation traditional lab-based lab-based othersample results rapid retestingoral fluid (7) HIV-1 EIA r/r (3/7) N/A Unconfirmed reports ofHIV-1 W Blot Ind. (3) seroconversion outside PH testing HIV-1 EIA nr (4/7) N/A N/A HIV-1 W Blot neg. (2) HIV-1 W Blot Ind. (1)serum (7) HIV-1/2 EIA nr (7/7) OraQuick pos. (3/7) <75 RNA copies/ml (1) HIV-1 W Blot neg. (7/7)* Unigold neg. (3) HIV-2 EIA nr (7/7) OraQuick neg. (4/7) Unigold neg. (3) Unigold n/a (1)All cases are being monitored for seroconversion, poor client return rates thus far. * One individual w/ initial W Blot Ind., negative on redraw
BBI Seroconversion Panel Results: G.S. G.S days since HIV-1/2 HIV-1/2 Unigold OraQuick Member# 1st bleed SP Plus O HIV-1r (20) (40) PRB958-01 0 0.1 0.25 N N N PRB958-02 2 0.1 0.25 N N NPRB958-03 7 0.1 0.2 N N NPRB958-04 9 0.1 0.2 N N NPRB958-05 15 1.0 2.4 N N NPRB958-06 17 2.6 11.0 wP N NBBI BOL BOL BOLC.B. W BlotRT-PCR PRB958-01 no bands 2 X 102 02 no bands 2 X 103 03 no bands 2 X 105 04 no bands 5 X 105 05 no bands 4 X 104 06 no bands >8 X 105BBI BBI
BBI Seroconversion Panel Results: G.S. G.S days since HIV-1/2 HIV-1/2 Unigold OraQuick Member# 1st bleed SP Plus O HIV-1r (20) (40) PRB959-01 0 0.1 0.2 N N N PRB959-02 7 0.1 1.0 N N NPRB959-03 9 0.2 7.0 N N NPRB959-04 14 1.8 13.1 P P PPRB959-05 19 7.3 13.1 P P PPRB959-06 21 7.6 13.1 P P P PRB959-07 267.8 13.1 P P PBBI BOL BOL BOLC.B. W BlotRT-PCR PRB959-01 no bands 2 X 105 02 no bands >8 X 105 03 no bands >8 X 105 04 p24, gp160 8 X 105 05 p24, gp160 5 X 105 06 p24, gp160 3 X 105 07 p24, gp160 >8 X 105 BBI BBI
Florida Lessons Learned (thus far): Altering our algorithm has improved rapid confirmation TAT. Is it advisable as numbers increase and testing sites vary? Follow up success on discordant cases is dependant on POC testing site. Ex. Jail settings are better than some PH clinics. Repeating rapid tests in the laboratory, if possible, on POC presumptive positive cases is a valuable tool in differentiating user vs. assay discordance. Sample choice in the confirmation process may limit additional testing needs. We clearly have discordance between rapid assays. Need for further investigations! We recommend enlisting CDC’s assistance early in the process.