Download
1 / 28
310 likes | 368 Views
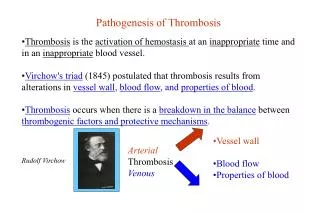
2. Pathogenesis of Viruses. INTRODUCTION TO VIRAL PATHOGENESIS Viral pathogenesis is the series of steps that occurs when a virus infects the host.

E N D
2 Pathogenesis of Viruses
INTRODUCTION TO VIRAL PATHOGENESIS Viral pathogenesis is the series of steps that occurs when a virus infects the host. The term pathogenesis refers to the processes related to disease induction; therefore, viral pathogenesis often refers to disease induction by a virus rather than the process of infection per se. However, viral infection does not always result in apparent or immediate disease, and the border between infection and disease becomes less clear as we learn more Viral pathogenesis is the integrated result of many complex factors unique to a particular virus, a particular species, and an individual host. The interplay of these factors determines the nature of infection, whether disease occurs, and the severity of disease.
DEFINITIONS AND CONCEPTS IN VIRAL PATHOGENESIS Productive, Abortive, and Latent Infection Infectionis the process by which a virus introduces its genome into a cell. Infection is productiveif new infectious virus is made and abortiveif no new infectious virus is produced. Infection is latent if the production of infectious virus does not occur immediately but the virus retains the potential to initiate productive infection at a later time. The process of reinitiating a productive infection cycle from the latent state is termed reactivation. Latency is not merely a slow productive replication cycle; latency represents a unique transcriptional and translational state where infectious virus is not present, but where a productive replication cycle can be reinitiated when the need arises. A cell is permissive if it can support productive infection and nonpermissive if infection cannot occur at all or is abortive.
Acute Versus Chronic or Persistent Infection Acute infection occurs when a virus first infects a susceptible host (Fig. 10.1). Chronic or persistent infection is the continuation of infection beyond the time when the immune system might reasonably be expected to clear acute infection. The cases, chronic infection may represent continuous replication, latent infection, abortive infection without clearance of residual nucleic acid, or perhaps some as-yet-unidentified form of viral infection. 256 |
In some cases, as for HBV or hepatitis C virus (HCV), a proportion of persons become chronically infected while others are cured. In these cases, the transition from acute to chronic is arbitrarily defined as the time when most patients have cleared acute infection. In other cases, essentially all hosts become chronically infected, as is seen with herpesviruses or lentiviruses such as human immunodeiciency virus (HIV). In this case, the transition between acute and chronic infection is defined as the time required for clearance of the initial burst of viral replication and establishment of equilibrium between the host and the virus. There are two primary mechanisms for establishment of chronic infection: continuous replication and establishment of latency. During latent viral infection, the virus has a genomic and transcriptional strategy, often involving restricted viral gene expression, which allows the genome to survive even when lytic replication is not occurring. Examples include the proviral form of retroviruses or the circular episomal form with selective expression of viral genes observed for herpesviruses such as Epstein-Barr virus (EBV) and herpes simplex virus (HSV). Often, latently infected cells express no viral proteins, making latency immunologically silent. This is the ultimate form of immune evasion, as the host has no known mechanisms for sensing the presence of the virus. To survive and spread from the latently infected cell, the virus must be able reactivate and reinitiate the lytic cycle of gene expression, potentially generating antigens that the immune system can respond to.
To succeed via continuous replication, a virus must generate new infectious virions despite ongoing innate and adaptive immune responses. Even for viruses that utilize the establishment of latency as a primary strategy, intermittent reactivation and replication may be required to maintain latency and to spread from host to host. Some viruses, such as HIV, persist via both continuous replication and establishment of latency, presenting a particularly dificult challenge for the host immune system.
Quasispecies The mixture of viruses present in the host at a given time is a quasispecies. Although it is convenient to think of a virus as a single homogeneous agent, this is not true because both viral RNA and DNA polymerases make errors that generate mutant viruses during infection. The polymerases of RNA viruses are generally less accurate in copying template molecules than those of DNA viruses; mutation may therefore play a greater role in RNA than DNA virus pathogenesis. Control of Acute Versus Chronic Infection The distinctions between acute and chronic or persistent infection are very important. The viral genes and host immunefactors that foster or control acute versus chronic infection are distinct. For example, the cytokine interferon-g (IFNg) regulates latency and continuous replication of the murine g HV68 (also referred to as MHV-68) but has at most a minimal effect during acute infection. This indicates that certain host responses are more relevant to chronic than acute infection. Many viruses, including herpesviruses, papillomaviruses, and retroviruses, use different gene or gene expression patterns to succeed during acute versus chronic infection. For these reasons, it is fundamentally important not to consider chronic infection as a mere continuation of acute infection.
Equilibrium and Nonequilibrium States in Pathogenesis A fundamental concept in pathogenesis is that acute infection is a nonequilibrium state, whereas chronic infection is a metastable equilibrium between virus and host. During acute infection, both the host response and virus infection change continuously until infection is resolved or progresses to death of the host or establishment of chronic infection. In contrast, chronic infection, once established, is an equilibrium process with viral and host processes balancing each other. In particular, the immune system of the host brings the acute infection under control and delays or prevents a chronic infection from killing the host.
Disease • Disease is a harmful pathologic consequence of infection. In many cases, infection is apparently harmless to the host and does not result in disease. One of the most important goals of pathogenesis research is to define in molecular terms what determines the difference between infection and disease. Even highly virulent viruses often establish infection in a greater number of hosts than they cause disease. Viruses such as rabies, Ebola, or HIV, which cause significant disease in nearly all infected persons, are the exception. • Disease may be associated with: • cell and tissue destruction (as in rabies virus killing neurons) • induction or secretion of inflammatory cytokines (as in the induction of fever by many viruses), • cellular dysfunction induced by viral infection (as in the case with lymphocytic choriomeningitis virus [LCMV] infection of the pituitary), • paracrine effects of viral gene products (as in induction of angiogenesis by Kaposi’s sarcoma herpesvirus [KSHV]) • induction of malignant tumors to the effects of the immune system as it responds to infection (as in immunopathology seen with many viruses) • the presence of a specific virus interacting with allelic polymorphisms in the host to trigger disease.
In many cases, virus-associated disease is defined as a series of nonspecific symptoms or signs such as fever, malaise, or anorexia. The presence of these symptoms and signs is common to infection with many different pathogens and therefore provides little insight into the mechanisms of viral pathogenesis. Recent work with microarray technology suggests that even the non- specific syndromes associated with acute virus infection with different viruses may be distinguished by the pattern of host gene expression. It is likely that pathogenesis researchers will use such molecular signatures to distinguish between infections with different viruses and to define host genes involved in viral pathogenesis. In contrast to the nonspecific syndromes commonly associated with virus infection, the presence of specific symptoms or signs of disease such as hepatitis, immunodeficiency, pocks on the skin, or paralysis provides important clues as to the nature of the pathogenic process.
Virulence Virulence—the relative capacity of a virus to cause disease— determines the relationship between infection and disease. Virulent viruses cause disease in a greater proportion of infected hosts, and cause more severe disease, than viruses of lower virulence. Virulence comes in many forms, from the induction of rapid death as for variola major (the causative agent in smallpox) to the induction of tumors over prolonged periods, as is the case with certain papillomaviruses or herpesviruses, to the induction of organ failure over many years, as is the case with chronic HBV or HCV infection. Thus, the manifestations of virulence highly depend on the strategies that a given virus uses during infection. virulence is properly used to compare the disease-inducing capacity of related viruses, such as different strains of the same virus. Other aspects of pathogenesis, including tropism, the host response to infection, and interactions between the virus and host tissues, play key roles in viral virulence. Invasiveness Invasiveness is the capacity of a virus to enter into and damage a tissue, a property that distinguishes viruses with high potential virulence but differ in the efficiency with which they enter target tissues. For example, a virus may be highly virulent if directly inoculated into the central nervous system (CNS) but unable to cause disease if inoculated into the periphery, whereas a related virus with a mutation allowing it to cross the blood– brain barrier into the CNS can cause lethal disease following either peripheral or intracranial inoculation
Evasion of Host Molecules and Mechanisms Most viruses have evolved mechanisms to counter host innate and adaptive immunity or to bypass intrinsic cellular resistance molecules so that the virus can complete the infectious process and spread to a new host. These mechanisms constitute viral evasion of host responses. Often, evasion strategies involve viral genes with close homology to host genes, as when a virus encodes a host cytokine or cytokine receptor mimic. Other evasion strategies utilize molecules with novel structures to avoid host responses. Because the mechanisms responsible for acute and chronic infection differ, both with regard to viral and host factors, it follows that immune evasion mechanisms are different for acute versus chronic infection. During acute infection, viral immune evasion strategies commonly focus on the host innate immune response, whereas evasion of adaptive immunity is more important for maintaining chronic infection.
Tropism Tropism is the capacity of a virus to infect or damage specific cells, tissues, or species. It is a fundamentally important contributor to viral pathogenesis and virulence, as the capacity to induce disease depends on the cell and tissue infected. For example, a neurotropic virus such as West Nile Virus can cause encephalitis or paralysis, whereas a virus with tropism for CD4 T cells such as HIV causes immunodeficiency. One key determinant of viral tropism is the cognate interaction between the viral cell attachment protein(s) and receptor(s) present on host cells. However, there are many additional factors that determine cell, tissue, and species tropism. Essential Genes, Virulence Genes, and Virulence Determinants Virulence is determined by the capacity of a virus to grow, be invasive, infect vulnerable cells, evade the immune system, subvert cellular processes, and cause tissue damage. These capacities are encoded in the viral genome, by alleles of individual virulence genes. Virus particles can contain virulence determinants that are not encoded in their genomes. For example, vaccinia virus incorporates host complement regulatory proteins into its envelope, thereby becoming resistant to inactivation by host complement proteins.
The stages in poliovirus pathogenesis are outlined in Figure 10.2. The virus enters the intestine via the fecal–oral route, binds to M cells overlying the Peyer’s patch, is transported into the intestinal wall, and then replicates in lymphoid cells, leading to a primary viremiaand infection of secondary sites. Replication in secondary sites gives rise to a secondary viremia that reaches a level capable of initiating CNS infection. CNS infection involves passage of the virus across the blood–brain barrier to infect neurons within the CNS. The blood–brain barrier is viewed as an important anatomic barrier to infection of the CNS, and passage across this barrier is poorly understood. Alternatively, the virus may spread via the blood to peripheral nerves and then spread up the nerves to enter the CNS. Within the CNS, the virus infects motor neurons; destruction of these cells leads to paralysis. Certain motor neurons are hypothesized to more susceptible to poliovirus infection than others, and some poliovirus strains are either more invasive or more likely to kill neurons than others; these variables contribute to variation in disease penetrance and severity.
Conceptualizing Viral Pathogenesis as the Integrated Effects of Host Genetic Variation It has been clear since the earliest studies of viral pathogenesis that hosts differ significantly in genetic susceptibility to infection. The major host determinant of viral virulence and pathogenesis is innate and adaptive immunity, but host genes not involved immunity also play a role. Allelic variations in these host genes can alter viral pathogenesis (Fig. 10.5).
DETERMINANTS OF CELL, ORGAN, AND TISSUE TROPISM One of the most important concepts for understanding pathogenesis is the concept of cell, organ, and species tropism. Tropism is determined by many factors in both the virus and the host, including how the virus enters the host, how the virus spreads within the host (lymphatic, neural, or hematogenous spread), the permissiveness of specific cell types for the virus (as defined by receptors, cellular differentiation, and intrinsic cellular resistance to infection), the nature of innate and adaptive immune responses, and specific properties of tissues such as accessibility and effectiveness of the immune system (immunoprivilege). Each of these factors can play a determining role during viral infection and must be considered when defining mechanisms of viral pathogenesis.
Entry into the Host A virus must access permissive cells to establish infection and therefore must overcome a series of anatomic and innate immune barriers to enter the host. The route of entry and the mechanisms of spread are therefore important determinants of viral tropism. The route and tissue through which a virus infects the host may be clear from epidemiologic studies. For example, both measles virus and VZV spread by the respiratory route, and polioviruses and noroviruses spread fecal–orally. However, even when the route of infection is known, the precise events involved in entry into the host are mostly unknown. The critical determinants of viral spread include the form of the virus that spreads, the capacity of the virus to survive in the environment, the route of natural exposure to the virus, the mechanisms by which the virus gains entry, and the nature of host barriers to infection.
Viruses may enter the body in different forms and via different vehicles. • The viral strategy for overcoming host barriers to entry is tightly linked to the form of the virus that spreads and how the virus is shed from the previously infected host. • For example, viruses may enter • carried in infected cells, • may be injected via the mouth parts of arthropods, • may be contained in droplets or fomites shed from an infected host, • or may be ingested as free virus. • To spread in a population, viruses may benefit from survival in the environment. For example, HIV is relatively unstable in the environment and does not effectively spread via environmental surfaces. This contrasts dramatically with noroviruses such as Norwalk virus that can spread via contact with contaminated environmental surfaces. • There are six primary portals of entry for viruses, each used by a variety of viruses. Five of these are epithelial surfaces: skin, conjunctiva, respiratory tract, gastrointestinal tract, and genitourinary tract. The sixth is the unique interface between the mother and the germ cell or the developing fetus.
Penetration Through Epithelial Barriers The body is covered by epithelia, presenting a large surface for viruses to access. However, epithelia share several properties that inhibit viral entry. For example, epithelial cells are constantly turning over and being replenished; thus, cells that are contacted by a virus are shed continuously. The skin has an added protective mechanism, being many cells deep with the surface comprised of metabolically inactive cells that cannot support viral replication. In addition, barriers may be protected by low pH or secretions, including mucus. Epithelial tissues are highly active immune organs. In all epithelia, DCs (e.g., Langerhans cells in the skin) serve as sentinels for invasion, having the capacity to, when activated, move to lymph nodes to induce immune responses. These sentinel cells play a dual role in infection, both as critical for induction of immunity and as cells targeted by viruses as an initial site of infection. Intraepithelial lymphocytes are present in subepithelial and epithelial tissues, providing cells capable of protective immune responses in the most superficial layers of the body. In addition, epithelial cells themselves may be activated to express interferons or other antiviral molecules. In many sites, an invading virus is subject to inactivation by antibodies and complement. Even when a virus passes superficial epithelial barriers, the virus must confront the innate and adaptive immune response as well as an increasingly well understood set of intracellular barriers to infection collectively referred to as intrinsic cellular resistance to infection.
Vertical Spread of Viruses Many viruses infect either the immature fetus or the newborn e Viruses cross epithelial barriers through mechanical breaches (e.g., vectorborne delivery of arboviruses or bite wound delivery of rabies) or by accessing specialized cells during the birth—a process referred to as vertical transmission. There are two mechanisms for entry into the developing fetus. The first is via placental penetration, as when a virus enters the fetus after invasion of the fetal circulation or amniotic fluid. Viruses such as HCMV and rubella can spread transplacentally, with devastating consequences for the developing fetus. Viruses such as human endogenous retroviruses (HERVs) can also be vertically transmitted via the germ line and constitute a significant fraction of the human genome.HERVs continue to proliferate within the genome and are likely to exert both beneficial and detrimental effects on their hosts. Systemic Spread of Virus Infection Once a virus has passed through epithelia or penetrated the placenta, the virus may still be far from its target cells and tissue(s). Viruses spread via three host systems that can provide access to a large number of tissues and cells: blood, lymphat- ics, and nerves. Although the blood is a major highway for spread of viruses through the host, many viruses use nerves or a combination of hematogenous and neural spread to access host tissues. The level of viremia has been correlated with the severity of acute viral disease, the prognosis of chronic viral disease (as in HIV), the extent of viral dissemination, and the eficiency of viral spread between hosts.198,307 The level of viremia is a func- tion of viral access to the blood, viral clearance from the blood, and the vehicle (plasma vs. cell associated) that the virus uses to travel through the blood. Viruses can access the blood either directly via introduction into the circulation, as by a needle or an insect bite, or indirectly after entering into and replicat- ing in tissues. A very common inding is the rapid appearance of a virus in draining lymph nodes or in lymphoid structures such as Peyer’s patches or tonsils. The connection between viral spread to lymphoid structures and subsequent spread to the rest of the host was recognized early on.73,182 Entry into lymphoid tissue is a two-edged sword for the virus, as a facile route to access the viscera of the host but one that passes through the very tissues that generate adaptive antiviral immune responses. For viruses that primarily infect mucosal surfaces such as inluenza virus, rotavirus, papilloma- viruses, rhinoviruses, and noroviruses, it is likely that the pri- mary effect of entry into the lymphoid system is the induction of antiviral immune responses. However, there are clear advan- tages for lymphoid invasion if the virus has tropism for cells of the immune system that are capable of circulating and enter- ing tissues. For example, HIV and EBV each have tropism for lymphocytes for latent and/or productive infection, and both MCMV and HCMV can spread through the body in infected cells of the monocyte-macrophage lineage.
In many cases, viruses can access the nervous system by infecting neurons in the periphery and then spreading along e axons toward the CNS.198 The classical example of this strat- egy is rabies virus, which spreads along nerves from the area of inoculation to the CNS.131 The time between inoculation and development of signs and symptoms of rabies encepha- litis depends on the length of the nerves between the site of inoculation and the CNS. The virus travels up nerves toward the CNS at a rate of 50 to 100 mm/day, and the disease can be cured by surgical removal of the infected limb as long as the virus has not entered the CNS.13,131 For example, if the initial bite is on a lower extremity, there is a longer time within which vaccination and passive transfer of rabies-immune anti- body can be effective than if the bite is on the face.131 Studies with several viruses, including HSV, pseudorabies virus, and reoviruses, have been used to elucidate the viral and cellular determinants that regulate viral spread through neural tissues, including sophisticated genetic and molecular mechanisms that regulate viral anterograde and retrograde axonal trans- port. Importantly, the immune system can also modulate neu- ral spread. For example, antibodies can interrupt many of the steps in neural spread of reoviruses to and within the CNS (Fig. 10.8). Refer to the eBook for an expanded discussion of the mechanisms of neural spread of viruses.
Determinants of Cell, Tissue, and Species Tropism Once a virus has spread via lymphatic, hematogenous, or neu- ral routes, a fundamental determinant of viral pathogenesis becomes the distribution of the virus between and within tis- sues of the host. Distribution of virus in tissues is a dynamic process determined by competing processes, including the speed of viral replication, the presence of speciic viral receptors or other pro-viral factors the permit viral entry or replication, viral mutation rate, viral virulence genes, host susceptibility and resistance genes, and innate and adaptive immunity. It is useful to think of tissue distribution of a virus as an ongoing battle between the virus and the host being played out in dif- ferent tissues. This battle has very local aspects, such as the con- tact between a virus and a speciic cell or the contact between an NK cell or cytolytic T cell and a virus-infected cell. How- ever, the outcome of this battle is also determined by effects over short distances in tissues, as, for example, the effects of host cytokines or virus-encoded soluble proteins that evade or subvert host responses. Lastly, there are long-range effects of host responses on infection, including production of antibody, synthesis of stress steroids, activation of the bone marrow to produce inlammatory cells, stimulation of the liver to syn- thesize and release acute-phase reactants such as complement proteins, and stimulation of autonomic centers in the brain to produce fever. The Role of Viral Receptors in Cell, Tissue, and Species Tropism An important step in viral infection, and a primary determi- nant of the distribution of virus between and within tissues, is the interaction of a virus with speciic receptors on permissive cells. Receptor expression plays a major role in determining the tropism of several viruses, including poliovirus and measles virus, and the use of molecular tools, including transgenic mice, expressing the virus-speciic receptors provides key insights into the role of receptors in regulating viral tissue tropism and pathogenesis. The importance of viral–receptor interactions is further illustrated by the fact that zoonotic viruses must often adapt to receptors in their new host species to effectively cause disease and disseminate, as was the case with SARS.161 These binding interactions are necessary for infection but are often not suficient to explain all aspects of cell, species, and tissue tropism. For example, CD4 and chemokine receptors such as CCR5 or CXCR4 confer susceptibility to HIV infection; how- ever, permissiveness is also controlled by cytoplasmic proteins that restrict HIV infection. Often, viruses use a binding receptor to increase the con- centration of virus at the cell surface and one or more entry receptors. An example of this latter strategy is HSV, which interacts with speciic sulfated sugars on heparan sulfate255 in a process that enhances infection but is not required if a cell expresses an entry receptor such as the appropriate nec- tin.88,263,269 Another example of this strategy is utilized by serotype 3 reoviruses, which interact with sialic acid via one portion of their cell attachment protein s1 and the protein JAM1 via another portion of the s1 protein.54 Importantly, the interaction with the broadly expressed carbohydrate sialic acid has been shown to be important in the tropism of the reovi- rus in vivo, indicating that even interactions with ubiquitously expressed molecules can play a role in cell and tissue tropism.54 e Tropism can also be conferred by interactions between viral cell attachment proteins and proteases, as is seen with Newcas- tle disease and inluenza viruses.41,191 Refer to the eBook for a more extensive discussion of how receptor tropism affects viral pathogenesis using poliovirus infection as an example
Innate Immunity and Intrinsic Cellular Resistance to Infection Determine Tropism Factors in addition to speciic receptors play a major role in determining viral tropism. Tropism can be determined by pro- teins responsible for cell-intrinsic defense against viral infection, transcription factors, cell cycle regulators, and microRNAs. For example, the liver-speciic host microRNA miR-122 is essen- tial for robust HCV replication,137 and inhibition of miR-122 in nonhuman primates limits HCV replication.151 Once a virus has bound to a cell and delivered its genome or capsid to the cytoplasm, a series of events occur that can have a profound effect on the viral cell tropism. These events likely explain why receptor expression does not always explain the cell and tissue tropism of a virus. The host cell expresses on its cell surface and in its cytoplasm molecules that can either directly inhibit viral replication (intrinsic cellular resistance to infection) or can induce a signaling cascade that in turn gener- ates antiviral molecules (innate immune responses). Together, these molecules and pathways are determinants of both the permissiveness of cells for viral replication and species tropism. It is likely that mechanistic relationships will be discovered between molecules involved in innate immunity and intrinsic cellular resistance to infection as more is learned about each of these two important processes. Molecules involved in innate immunity can be important components of tissue and species tropism. This is illustrated by myxoma virus, which does not normally infect mice but read- ily infects murine cell lacking type I interferon responses and causes lethal disease in STAT-1 deicient mice.305 Intrinsic cel- lular resistance to infection is also conferred by molecules such as the TRIM or APOBEC proteins that restrict retrovirus infec- tion. Importantly, allelic variations in the genes involved in these processes may contribute to regulation of viral pathogenesis.
Viral Disease • Some persistent viruses are oncogenic • Several viruses can cross the placenta causing developmental disturbances and permanent defects – teratogenic • Diagnosis of viral diseases –symptoms, isolation in cell or animal culture, serological tests for antibodies; some tests for antigens
Viruses and Cancer • Tumor • growth or lump of tissue; • benign tumors remain in place • Neoplasia • abnormal new cell growth and reproduction due to loss of regulation • Anaplasia • reversion to a more primitive or less differentiated state • Metastasis • spread of cancerous cells throughout body
Carcinogenesis • Complex, multistep process • Often involves oncogenes • cancer causing genes • may come from the virus OR may be transformed host proto-oncogenes (involved in normal regulation of cell growth/differentiation)
Possible Mechanisms by Which Viruses Cause Cancer • Viral proteins bind host cell tumor suppressor proteins • Carry oncogene into cell and insert it into host genome • Altered cell regulation • Insertion of promoter or enhancer next to cellular oncogene