Download
1 / 33
350 likes | 681 Views
Coronary Circulation. Dr. Meg- angela Christi Amores. Physiologic Anatomy. main coronary arteries lie on the surface smaller arteries then penetrate from the surface into the cardiac muscle mass. Physiologic Anatomy.

E N D
Coronary Circulation Dr. Meg-angela Christi Amores
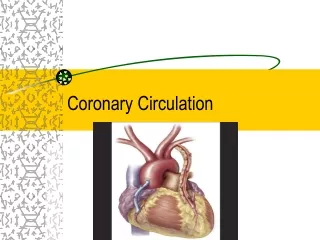
Physiologic Anatomy • main coronary arteries lie on the surface • smaller arteries then penetrate from the surface into the cardiac muscle mass
Physiologic Anatomy • left coronary artery supplies mainly the anterior and left lateral portions of the left ventricle • right coronary artery supplies most of the right ventricle as well as the posterior part of the left ventricle
Coronary Circulation • coronary venous blood flow from the left ventricular muscle returns by way of the coronary sinus • most of the coronary venous blood from the right ventricular muscle returns through small anterior cardiac veins
Variations in Blood Flow in Different Tissues and Organs The resting coronary blood flow in the human being averages about 225 ml/min
Coronary Circulation • In exercise, heart in the young adult increases its cardiac output fourfold to sevenfold • Work output of heart increases 6 – 9fold • Coronary blood flow increases 3 – 4fold • "efficiency" of cardiac utilization of energy increases to make up for the relative deficiency of coronary blood supply
coronary capillary blood flow in the left ventricle • muscle falls to a low value during systole • reason for this is strong compression of the left ventricular muscle around the intramuscular vessels during systolic contraction.
Control of Coronary Blood Flow • Local Muscle Metabolism • Primary controller of coronary blood flow • local arteriolar vasodilation in response to cardiac muscle need for nutrition • whenever the vigor of cardiac contraction is increased, regardless of cause, the rate of coronary blood flow also increases
Control of Coronary Blood Flow • Oxygen Demand • Blood flow in the coronaries usually is regulated almost exactly in proportion to the need of the cardiac musculature for oxygen • 70 per cent of the oxygen in the coronary arterial blood is removed as the blood flows through the heart • coronary blood flow does increase almost in direct proportion to any additional metabolic consumption of oxygen
Mechanism • decrease in the oxygen concentration in the heart causes vasodilator substances to be released • very low concentrations of oxygen in the muscle cells, large proportion of the cell's ATP degrades to adenosinemonophosphate • further degraded and release adenosine into the tissue fluids of the heart muscle • resultant increase in local coronary blood flow
Nervous Control Of Coronary blood Flow • Stimulation of AUTONOMIC nerves • Affect coronary blood flow DIRECTLY and INDIRECTLY • Direct: • Acetylcholine from VAGUS nerves and EPINEPHRINE or NOREPINEPHRINE from sympathetic nerves • Indirect: • secondary changes in coronary blood flow caused by increased or decreased activity of the heart • Plays more important role in NORMAL control
Direct effect on Coronary Vasculature • acetylcholine released by parasympathetic stimulation has a direct effect to dilate the coronary arteries • distribution of parasympathetic (vagal) nerve fibers to the ventricular coronary system is not very great • more extensive sympathetic innervation
Direct effect on Coronary Vasculature • sympathetic transmitter substances norepinephrine and epinephrine can have either vascular constrictor or vascular dilator effects, depending on the presence or absence of constrictor or dilator receptors • constrictor receptors -alpha receptors • dilator receptors - beta receptors • epicardial coronary vessels have a preponderance of alpha receptors
Special Features of Cardiac Muscle • under resting conditions • consumes fatty acids to supply most of its energy instead of carbohydrates • under anaerobic or ischemic conditions • must call on anaerobic glycolysis mechanisms for energy • Consumes large amounts of glucose • Forms large amounts of LACTIC ACID - causes of cardiac pain
Ischemic Heart Disease • HYPOXEMIA vs ISCHEMIA • What is hypoxemia? • Decreased oxygen concentration in the blood • What is ischemia? • Diminished coronary blood flow
Ischemic Heart Disease • most common cause of death in Western culture • results from insufficient coronary blood flow • Atherosclerosis is most frequent cause • people who eat excessive quantities of cholesterol • Sedentary lifestyle • large quantities of cholesterol gradually become deposited beneath the endothelium • invaded by fibrous tissue and frequently become calcified
Ischemic Heart Disease • Acute coronary occlusion • most frequently occurs in a person who already has underlying atherosclerotic coronary heart disease • The atherosclerotic plaque can cause a local blood clot called a thrombus • clot breaks away from its attachment on the atherosclerotic plaque – embolus • that local muscular spasm of a coronary artery also can occur
Collateral Circulation • In a normal heart, almost no large communications exist among the larger coronary arteries • anastomoses do exist among the smaller arteries sized 20 to 250 micrometers in diameter
When a sudden occlusion occurs in one of the larger coronary arteries, the small anastomoses begin to dilate within seconds • diameters of the collateral vessels do not enlarge much more for the next 8 to 24 hours • collateral flow does begin to increase, doubling by the second or third day and often reaching normal or almost normal coronary flow within about 1 month
When atherosclerosis constricts the coronary arteries slowly over a period of many years rather than suddenly, collateral vessels can develop at the same time while the atherosclerosis becomes more and more severe
Myocardial Infarction (MI) • area of muscle that has either zero flow or so little flow that it cannot sustain cardiac muscle function is said to be infarcted • after infarction occurs, small amount of collateral blood seeps, lead to overfilling of stagnant blood • LAST amount of oxygen is used, • Muscle becomes bluish
Causes of death after MI • (1) decreased cardiac output; • (2) damming of blood in the pulmonary blood vessels and then death resulting from pulmonary edema; • (3) fibrillation of the heart; and, occasionally, • (4) rupture of the heart
Cardiogenic shock • heart becomes incapable of contracting with sufficient force to pump enough blood into the peripheral arterial tree • always occurs when more than 40 per cent of the left ventricle is infarcted • death occurs in about 85 per cent of patients
Damming of venous blood • Mostly in the lungs • acute pulmonary edema
Fibrillation of ventricles • Tendency is great if the infarct is large • Dangerous times: • during the first 10 minutes after the infarction • 1 hour or so later and lasting for another few hours • Causes: loss of K, injury current, powerful sympathetic reflex, cardiac muscle weakness dilates ventricles
Rupture of infarcted area • dead muscle fibers begin to degenerate • heart wall becomes stretched very thin • systolic stretch becomes greater and greater until finally the heart ruptures • Lead to cardiac tamponade • compression of the heart from the outside by blood collecting in the pericardial cavity
MI • Normally, a person cannot "feel" his or her heart • ischemia causes the muscle to release acidic substances, such as lactic acid
Angina Pectoris • hot, pressing, and constricting Cardiac pain that appears with exertion • whenever the load on the heart becomes too great in relation to the available coronary blood flow • felt beneath the upper sternum over the heart • Radiates to left arm and left shoulder but also frequently to the neck and even to the side of the face
Surgical Treatment • Aortic-Coronary Bypass Surgery • Coronary Angioplasty