Download
1 / 32
330 likes | 614 Views
Palpation. Usually inspection and palpation are discussed together because there is an intimate relationship between these two processes in the heart examination. Palpation not only confirms the results in inspection, but also discovers diagnostic signs.

E N D
Palpation Usually inspection and palpation are discussed together because there is an intimate relationship between these two processes in the heart examination. Palpation not only confirms the results in inspection, but also discovers diagnostic signs.
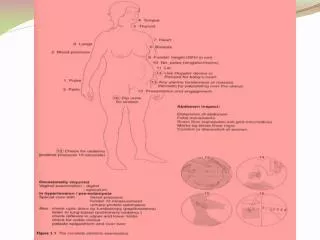
Through careful palpation, the examiner should aim to determine the location and size of the cardiac apex impulse, characterize its contour, and identify any abnormal precordial pulsations.
The various disturbances in rate(心率) and rhythm(心律) which have been observed can be confirmed by palpation.
Palpation gives us a better impression of the force of the heart beat than does inspection.
The palm of the hand, ventral surface of the proximal metacarpals, and fingers should all be used for palpation because each is useful for optimal appreciation of certain movements.
Apical impulse(心尖搏动) location duration amplitude intensity frequency regularity
Sustained sensation(抬举性搏动): LVH Forceful, sustained, through systole with great amplitude more than 2cm diameter
Precordial lift or heavy: RVH Decrease amplitude: myocarditis Massive pericardial effusion: impulse cannot be palpable
Thrill Thrill are palpable murmurs some what similar to the sensation on the throat a purring cat. Thrills are actually palpable fine vibrations, most commonly produced by blood from one chamber of the heart to another through a restricted or narrowed orifice, it may occur in systole, diastole, presystole and at times may be continuous.
Any thrill should be described as to its location, its time in cardiac cycle, and its mode of extension or transmission.
The intensity of the thrill varies according to the velocity of the blood, the degree of narrowing of the orifice and which it is produced and difference in pressure between the two chambers of the heart.
Quality of a thrill depends on the frequency of vibration producing it, rapid vibrations result in fine thrills whereas slower vibrations produce coarser thrill.
Restricted or narrowed orifice thrill according blood velocity Intensity degree of narrowing to gradient between two chambers
depends quality frequency on frequency: rapid fine thrill slow coarser thrill
Diastolic thrill The diastolic thrill felt near the apex is pathognomic of mitral stenosis(二狭). It may be compared quit accurately to the vibration which accompanies the sound of satisfaction which a cat makes.
It is usually felt only over a small area at or near the point of maximum impulse. It may not be felt when the patient is lying quietly in bed,
but may be brought out by moving the patient up and down rather rapidly a few times and thus producing more active cardiac contractions, and also by turning the patient on his left side.
Systolic thrill A systolic thrill may be felt over the precordium with its maximum intensity at the aortic area in aortic stenosis(主狭). This thrill is usually rough and purring, and commonly of greater intensity than any other thrill felt over the heart.
This systolic thrill of aortic stenosis is felt in the carotid(颈动脉) and brachial (臂动脉) arteries and its transmitted in the direction of the blood flow.
Systolic thrill In pulmonary stenosis(肺动脉瓣狭窄) a rough systolic thrill is felt over the pulmonary area and from here is transmitted upward and diagonally toward the left clavicle.
Systolic thrill In aneurysm of the ascending aorta(升主动脉瘤), which produces a definite area of pulsation, a systolic thrill may be felt over this area.
duration location disease systole second right ICS AS second left ICS PS third fourth left ICS VSD diastole apical area MS continuous 2nd left ICS PDA
Pericardial friction rub Pericardial friction rub(心包摩擦感) is a to-and-fro grating sensation, which is usually present during both phases of cardiac cycle, often rubs are more readily palpated with the patient sitting erect and leaning forward during the end period of deep inspiration.
The rub is caused by a fibrinous pericarditis(纤维素性心包炎). In the presence of pericardial effusion the rub will usually disappear because of the separation of visceral and parietal layers by the accumulated fluid.
Review • Method of palpation • Precordial pulsantion: LVH, RVH, myocarditis, massive pericardial effusion • Mechanism of thrill • Clinical significance of precordial thrill
单选题 震颤的论述,错误的是 A. 在心尖区触及收缩期震颤可见于二狭 B. 临床上凡触及震颤均可认为心脏有器质性病变 C. 触诊有震颤的部位多数可听到杂音 D. 在胸骨右缘第2肋间触及收缩期震颤可见于主狭 E. 在胸骨左缘第2肋间触及收缩期震颤可见于肺动脉瓣狭窄
心包摩擦感的论述,错误的是 A.为心脏收缩时脏层与壁层心包相互摩擦而产生 B. 随渗液的增多,心包脏层与壁层分离时摩擦感消失 C. 多在心前区或胸骨左缘第3、4肋间触及 D. 以收缩期、前倾体位更为明显 E. 以吸气末更为清楚
标准配伍型题 A. 胸骨左缘第二肋间收缩期震颤 B. 胸骨左缘3~4肋间收缩期震颤 C. 胸骨左缘第二肋间连续性震颤 D. 心尖区舒张期震颤 E. 胸骨右缘第二肋间收缩期震颤 主动脉瓣狭窄? 肺动脉瓣狭窄? 动脉导管未闭? 二尖瓣狭窄?