Download
1 / 25
400 likes | 858 Views
Introduction to Antibody Drug Conjugates (ADC) John Milne PhD, NIBRT 20 th June 2014. Paul Ehrlich (1854-1915). Ehrlich reasoned that if a compound could be made that selectively targeted a disease-causing organism, then a toxin for

E N D
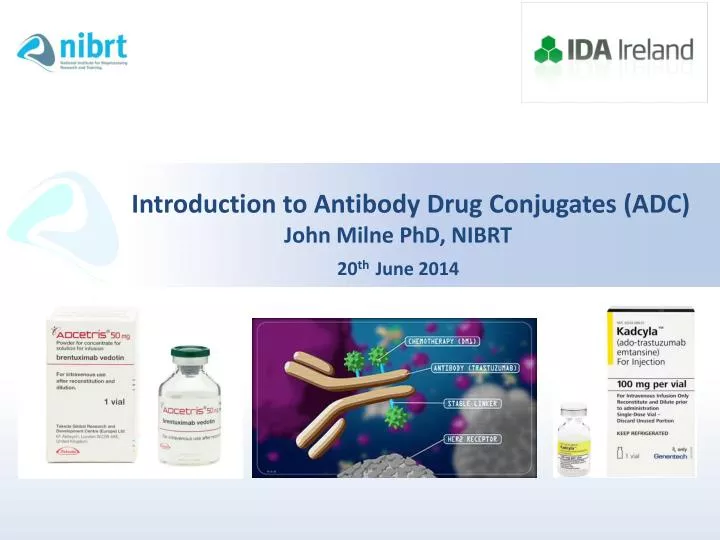
Introduction to Antibody Drug Conjugates (ADC)John Milne PhD, NIBRT20thJune 2014
Paul Ehrlich (1854-1915) • Ehrlich reasoned that if a compound could be made that • selectively targeted a disease-causing organism, then a toxin for • that organism could be delivered along with the agent of selectivity. • Hence, in 1913 he coined the phrase "magic bullet" (magischeKugel), • his term for an ideal therapeutic agent that could be created that killed • only the organism targeted. • The concept of a "magic bullet" was to some extent realized by the • invention of monoclonal antibodies as they provide a very specific binding affinity. • Principle of ADC technology – to selectively deliver payloads through an antibody • to enhance antibody activity and reduce systemic toxicity.
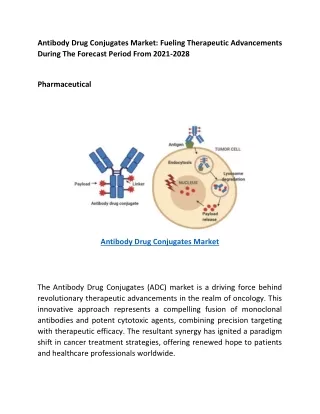
Antibody Drug Conjugates • Antibody Drug Conjugates (ADC) aim to take advantage of the specificity of monoclonal antibodies (mAbs) to deliver potent cytotoxic drugs selectively to antigen-expressing tumour cells. • The antibody (or fragment) is linked via a stable chemical linker, with a labile bond to a biologically active cytotoxic (anti-cancer) drug.
Approved ADC’s • Gemtuzumabozogamicin (Mylotarg®): Approved 2000. An anti-CD33 antibody conjugated to the cytotoxincalicheamicin: withdrawn from market in 2010. • Brentuximabvedotin (Adcetris®): Approved 2012; Takeda An anti-CD30 antibody conjugated via cleavable linker to cytotoxic monoethyl auristatin(MMAE) - Hodgkinslymphona and anaplastic large cell lymphona’s. • Ado-trastuzumabemtansine (Kadcyla®) Approved 2013; Genentech An anti-Her2 antibody conjugated via non-cleavable linker to cytotoxic “DM-1” (derivative of maytansine) - Her2 metastatic breast cancer.
Licensed ADC Products Emerging classes of armed antibody therapeutics against cancer Hess et al., Med. Chem. Commun., 2014, Advanced Article
Growth Potential • Market for ADC’s predicted to grow significantly • 18 of Top 20 Pharma involved in ADC Development. • 50+ ADC molecules in clinical trials. • Molecules in Phase I account for 70% of ADCs in clinical development. • Global sales of ADC - $500M by 2016. • The complexity of the ADC molecules adds to the uncertainty in the market. • There are opportunities for pharmaceutical companies to replenish their diminishing pipelines and gain first mover advantage in the market. • There have been several technological developments in the recent past with more stable linkers and potent cytotoxins allowing the development of next generation ADCs with improved safety/efficacy profile. Adapted from “Antibody Drug Conjugates Market 2013-2023”, Roots Analysis, Business Research and Consulting.
The ADC space: selected deals of interest • Deals typically also include an undisclosed single-digit percent of sales that is paid to the • licenser for any ADC from the collaboration that makes it to market. Data taken Zolotet al., (2013)., Nature Reviews Drug Discovery 12, 259-260
Antibody Drug Conjugates • The concept of ADCs appears simple, however the development of efficacious products is a considerable challenge! • Many parameters have to be optimised for a successful ADC product; • ADC stability (the drug should not be released before the ADC reaches its in vivo target) • Pharmacokinetics (the drug should not confer an undesired accumulation in a non-target organ) • Retention of immunoreactivity • Efficient release of the active form of the drug at the site of disease
ADC Toolkit • ADC’s are constructed from three distinct components; • A mAb that is specific to a tumour antigen • A highly potent cytotoxic agent • A linker species that enables covalent attachment of the • cytotoxin to the mAb through either the protein or glycan • Pay Load can be; • Chemotherapeutic • Radioisotope • Cytokine • Protein based toxin
ADC Design • ADC success depends on optimisation of each building block; • Antibody • Linker • Drug • The antibody should target a well characterised antigen with high expression at the tumour site and low expression on normal tissue to maximise efficacy. • Bifunctional linkers with attachment sites for both the antibody and drug are used to join the two components. • Current linker attachment protocols rely on the modification of solvent accessible lysine or cysteine residues on the antibody, giving rise to ADC populations with variable DAR’s.
ADC Design • As low drug loading reduces potency and high drug loading can adversely affect pharmacokinetics, DAR can significantly affect ADC efficacy. • Crucially the selected linker must be stable in the circulation to minimise toxicity but also be cleaved rapidly after the ADC finds its target antigen. • After binding to the target antigen the ADC receptor complex is internalised and once inside the cell the drug is released; • Hydrolysis of the linker • Enzymatic cleavage of the linker • Degradation of the antibody
Drug Antibody (DAR) • The average number of drugs that are conjugated to the antibody is the most important quality attributes of an ADC. • The DAR determines the amount of “payload” that can be delivered to the tumour cell. • This can directly affect both safety and efficacy.
The Linker • The identity and stability of the linker is crucial to the success of an ADC. • The linker must be stable to allow the ADC to circulate in the bloodstream before reaching the tumour site without prematurely releasing the free “cytotoxic” drug and damaging normal tissue. • The linker should also be labile enough to release the free drug efficiently.
The Linker • Two main classes of ADC drug linker that use different mechanisms for release of the drug from the antibody • Cleavable linker • Non-cleavable linker • Class 1: Cleavable Linkers • Lysosomal protease sensitive linkers • Acid sensitive linkers • Gluthathione sensitive linkers • Class 2: Non-cleavable Linkers Ref: TeicherB A , and Chari R V Clin Cancer Res 2011;17:6389-6397
Cleavable Linkers • Lysosomal protease sensitive linkers • This strategy uses lysosomal proteases such as Cathepsin B that recognise and cleave a dipeptide bond to release the free drug from the antibody. • Valine-citrulline dipeptide linkers are common in this class • e.g. Adcetris(Seattle Genetics/Millennium). • Acid sensitive linkers • This strategy takes advantage of the low pH (pH ~5) within lysosomes to trigger hydrolysis of an acid labile group (hydrazone) within the linker to release the drug. • Glutathione sensitive linkers • This strategy exploits higher concentration of thiols such as glutathione within cells relative to the bloodstream. Disulphide bonds within the linker are stable in circulation but are reduced by intracellular glutathione to release the free drug.
Non-cleavable Linkers • This strategy depends on complete degradation of the antibody after internalisation of the ADC. • The free drug is released with the linker attached to an amino acid from the mAb. • Non-cleavable linker strategies are best applied to payloads that are capable of exerting their anti-tumour effect despite being chemically modified e.g. Kadcyla (trastuzumab-MCC-DM1) (Genentech/Immunogen). • One advantage of non-cleavable linkers is their greater stability in circulation compared with cleavable linkers.
The Drug Payload • Two main classes of ADC payload undergoing clinical evaluation. • Drugs that disrupt microtubule assembly and affect mitosis • Dolastatin 10-based auristatinanalogs (Adcetris) • Maytansinoids (Kadcyla) • Drugs that target DNA structure, bind the minor groove of DNA causing DNA double strand cleavage • Calicheamicinanalogs (Mylotarg) • These cytotoxic agents demonstrate at least 100-1000 fold greater potency in in vitro proliferation assays against a broad range of tumour cell lines compared with conventional chemotherapeutic agents. • High potency is crucial because only an estimated 1-2% of the ADC dose will reach the tumour site, resulting in low intracellular drug concentrations!!!
If the efficiency of each step is 50%, only 1.56% of the administered dose will reach the intracellular target. Ref: TeicherB A , and Chari R V Clin Cancer Res 2011;17:6389-6397
Summary: Efficacy of ADC • Critical to the efficacy of an ADC are; • the target site-specificity and binding properties of the antibody, • the in vitro and in vivo stability of the linker and drug species, • the potency of the drug • both the distribution and average number of drug species on the antibody (DAR) • These factors highlight the importance of; • understanding the physiochemical properties of ADC’s and • choosing the appropriate bioanalytical techniques to assess and monitor them during manufacturing and subsequent storage.
Conjugation • Conjugation typically involves a controlled chemical reaction with specific amino acid residues exposed on the antibody surface. • Selection of the appropriate drug-conjugation strategy significantly affects efficacy, Pharmacokinetics and tolerability. • Two types of conjugation • Chemical conjugation • Site-specific conjugation
Chemical Conjugation • A reactive moiety on the linker molecule is joined covalently to the antibody via an amino acid side chain, commonly the e-amino group of lysine. • Alternatively in a two-step process the surface lysines on the antibody are first modified to introduce a reactive group, such as a maleimide and then conjugated to the drug linker containing a reactive handle (e.g a thiol group), e.g. Kadcyla. • Alternatively a controlled reduction of existing disulphide bonds may liberate free cysteine residues on the antibody, which then react with a maleimide attached to the drug linker (e.g. Adcetris)
Conjugation • The random conjugation processes produce heterogeneous mixtures of conjugated species with variable DAR’s. • When lysines are used for conjugation, heterogeneity in overall charge can impact solubility, stability and pharmacokinetics. • Thus the clinical success of an ADC produced by random conjugation depends on robust manufacturing processes that provide the ability to monitor, control and purifyheterogeneous products
Site-Specific Conjugation • Next generation ADC’s are focused on homogeneous products derived via site-specific conjugation. • Three differing strategies; • Insertion of cysteine residues in the antibody sequence by mutation. • Insertion of an “unnatural” amino acid with a bio-orthogonal reactive handle • Enzymatic conjugation (utilising specificity of enzymes)