Download
1 / 62
690 likes | 1.39k Views
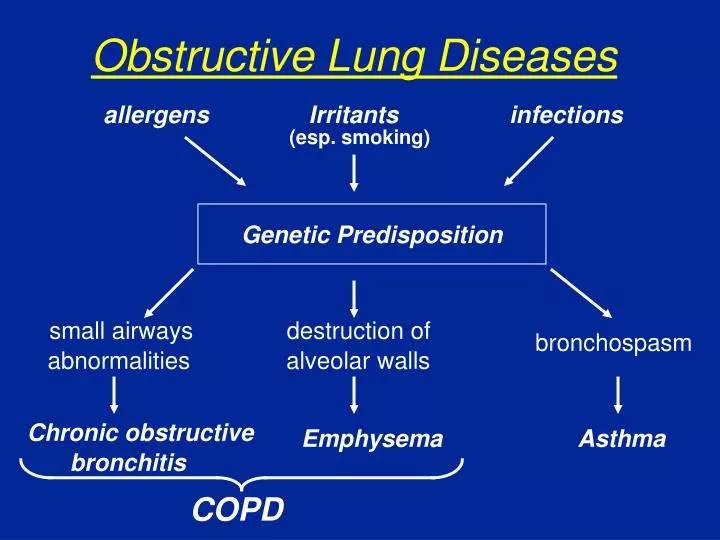
destruction of. small airways. alveolar walls. abnormalities. Chronic obstructive. bronchitis. Obstructive Lung Diseases. allergens. Irritants. infections. (esp. smoking). Genetic Predisposition. bronchospasm. Emphysema. Asthma. COPD. ASTHMA PATHOGENESIS. GENES. ENVIRONMENT.

E N D
destruction of small airways alveolar walls abnormalities Chronic obstructive bronchitis Obstructive Lung Diseases allergens Irritants infections (esp. smoking) Genetic Predisposition bronchospasm Emphysema Asthma COPD
ASTHMA PATHOGENESIS GENES ENVIRONMENT INFLAMMATION AIRWAY AIRWAY SYMPTOMS HYPERREACTIVITY OBSTRUCTION
destruction of small airways alveolar walls abnormalities Chronic obstructive bronchitis Obstructive Lung Diseases allergens Irritants infections (esp. smoking) Genetic Predisposition bronchospasm Emphysema Asthma COPD
Gross Appearance of Human Lung Normal Asthma Emphysema
PHARMACOLOGIC AGENTS • BRONCHODILATORS • Beta2-adrenergic agonists • Anticholinergics • Theophylline • Leukotriene modifiers • ANTI-INFLAMMATORY AGENTS • Corticosteroids • (Cromolyn/Nedocromil)
Bronchoconstriction Before 10 Minutes After Allergen Challenge
BETA-AGONISTS: ADVERSE EFFECTS • Tremor • Palpitations • Hypokalemia • Arrhythmias ?
PHARMACOLOGIC AGENTS • BRONCHODILATORS • Beta2-adrenergic agonists • Anticholinergics • Theophylline • Leukotriene modifiers • ANTI-INFLAMMATORY AGENTS • Corticosteroids • (Cromolyn/Nedocromil)
Comparison: Beta-agonists / Anticholinergics • Beta2-adrenergic agonists most effective bronchodilators in chronic asthma • Anticholinergics and beta2-adrenergic agonists effective in COPD • Anticholinergics often added to beta-agonists in acute asthma exacerbations • Tiotropium-long duration of action
Comparison: Beta-agonists / Anticholinergics • Beta2-adrenergic agonists most effective bronchodilators in chronic asthma • Anticholinergics and beta2-adrenergic agonists effective in COPD • Anticholinergics often added to beta-agonists in acute asthma exacerbations • Tiotropium-long duration of action
PHARMACOLOGIC AGENTS • BRONCHODILATORS • Beta2-adrenergic agonists • Anticholinergics • Theophylline • Leukotriene modifiers • ANTI-INFLAMMATORY AGENTS • Corticosteroids • (Cromolyn/Nedocromil)
THEOPHYLLINE • Mechanism of Action • Pharmacokinetics • Volume of distribution 0.5L/kg • Thus, 1 mg/kg increases serum level ~2 mcg/ml • Loading dose 5 mg/kg • Clearance • Liver • Differs not only between individuals but in same individual over time
THEOPHYLLINE • Mechanism of Action • Pharmacokinetics • Volume of distribution 0.5L/kg • Thus, 1 mg/kg increases serum level ~2 mcg/ml • Loading dose 5 mg/kg • Clearance • Liver • Differs not only between individuals but in same individual over time
Decreased Elimination Liver Disease Congestive Heart Failure Cor Pulmonale Ciprofloxacin Erythromycin Increased Elimination Cigarette Smoking Conditions and Drugs Affecting Theophylline Elimination
ASTHMA PATHOGENESIS GENES ENVIRONMENT INFLAMMATION AIRWAY AIRWAY SYMPTOMS HYPERREACTIVITY OBSTRUCTION
PHARMACOLOGIC AGENTS • BRONCHODILATORS • Beta2-adrenergic agonists • Anticholinergics • Theophylline • Leukotriene modifiers • ANTI-INFLAMMATORY AGENTS • Corticosteroids • (Cromolyn/Nedocromil)
Systemic Corticosteriods • Oral (usually prednisione) or parenteral (hydrocortisone, methylprednisolone) • Most effective therapy in serious exacerbations of asthma • Basically, any patient sick enough for hospitalization (and most that go to ER) treated with short course of systemic corticosteroid therapy
Cromolyn / Nedocromil • Anti-inflammaory effects in asthma, but minimal compared with inhaled corticosteroids • Mechanism of action poorly defined • Prevent mediator release from mast cells and other inflammatory cells • Can protect against allergen and exercise challenge • No adverse effects
PHARMACOLOGIC AGENTS • BRONCHODILATORS • Beta2-adrenergic agonists • Anticholinergics • Theophylline • Leukotriene modifiers • ANTI-INFLAMMATORY AGENTS • Corticosteroids • (Cromolyn/Nedocromil)
CYSTEINYL LEUKOTRIENES airway narrowing mucus secretion vascular leak 5-Lipoxygenase Pathway Membrane Phospholipids zileuton PG, TX AA FLAP 5-HPETE 5-LO LTC4 LTA4 synthase LTB4 LTC4 LTD4 LTE4 montelukast Cys LT1 zafirlukast
PEF or FEV1 PEF Variability Symptoms/Day Symptoms/Night Continual Frequent 60% >30% Daily >1 night/week >60% - <80% >30% >2/week but <1x/day >2 nights/month 80% 20% - 30% 2 days/week 2 nights/month 80% <20% Step 1 Mild Intermittent Stepwise Approach for Adults and Children (>5 years) Daily Medications Severity Class • Preferred treatment: • High-dose ICS + LABA AND, if needed, corticosteroid tablets or syrup long term Step 4 Severe Persistent • Preferred treatment: • Low-to-medium dose ICS + LABA Step 3 Moderate Persistent • Alternative treatment: Increase ICS dose within med dose range OR low-to-med dose ICS + LTM or theophylline • Preferred treatment: • Low-dose inhaled corticosteroid Step 2 Mild Persistent • Alternative treatment: cromolyn, LTM, nedocromil OR theophylline SR (serum concentration of 5-15 mcg/mL) • No daily medication needed Guidelines for the Diagnosis and Management of Asthma—Update on Selected Topics 2002. NIH, NHLBI. June 2002. NIH publication no. 02-5075.
Therapy of COPD • Symptomatic patients: bronchodilator • Anticholinergic or beta-agonist • Inhaled steroids in moderate-severe patients with multiple exacerbations • Acute exacerbations • Bronchodilators • Systemic corticosteroid - short course
RHINITIS • Inflammation of the nasal mucosa • Diagnosis • Rhinorrhea • Nasal blockage or stuffiness • Pruritus • Sneezing