Download
1 / 18
180 likes | 322 Views
CHILDREN’S COVERAGE: PAST, PRESENT & FUTURE Jeanne Lambrew, PhD Associate Professor, George Washington University Senior Fellow, Center for American Progress. February 15, 2007. OUTLINE. Creation and Implementation Structure & Accomplishments Issues in 2007.

E N D
CHILDREN’S COVERAGE:PAST, PRESENT & FUTUREJeanne Lambrew, PhDAssociate Professor, George Washington UniversitySenior Fellow, Center for American Progress February 15, 2007
OUTLINE • Creation and Implementation • Structure & Accomplishments • Issues in 2007
CREATION AND IMPLEMENTATION Context in 1997 • Gradual Expansion of Medicaid • In 1997, all poor children below the age of 13 were eligible nationwide • States used options, waivers to expand further • Wake of Bitter Battles: Failures to: • Cover to all Americans in 1993-94 • Block grant Medicaid in 1995 • New Term for President: Promised to: • Balance the budget and expand coverage for kids
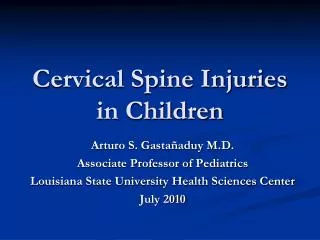
Uninsured Children in 1997 Distribution By Family Income As Percent of Poverty, 1997 32% 34% 63% of Insured Children 18% of Insured Children 34% 19% of Insured Children Source: Current Population Survey data, 1998, as described by the U.S. Department of Health and Human Services http://aspe.hhs.gov/health/98Chartbk/98-chtbk.htm
Conservative Opposition “Camel’s nose under the tent” Liberal Concerns Structure Funding (e.g., cuts in Medicaid) State Concerns Unfunded mandates Participation Who to Target Uninsured versus all low-income children What Type of Insurance Public versus private Comprehensive versus scaled-back benefits What Type of Financing Direct subsidies versus tax credits Entitlement versus block grants Challenges
New Title XXI States largely determine: How Who What Fed. gov’t provides: Protection for poor children Benefit standards Higher match to a cap Extend health coverage to uninsured children in families with: Too much income to qualify for Medicaid but Too little income to afford private insurance Do so in an “effective and “efficient manner” Compromise: SCHIP As Passed GOAL: MEANS:
STRUCTURE & ACCOMPLISHMENTSSnapshot • Type of Programs in 2006 • 11 Medicaid programs • 18 Separate programs • 21 Combination programs • Types Benefits in Separate Programs in 2003 • 21 Secretary-approved plans (including Medicaid benefits) • 14 State Employee Plans • 4 Largest HMO • 4 Federal Employees Health Benefit Plan
Upper Eligibility Limits for Children by State, July 2006 Of these, 9 States Already Covered Children up to 200% of Poverty When SCHIP Was Implemented 8 15 * 28 Note: Some states use income disregards, meaning that their upper eligibility limit exceeds 200% of poverty Sources: CMS, McClellan Testimony, July 2006
Enrollment in Medicaid & SCHIP, 1997-2004 Of 6.2 Million in SCHIP in 2004: - 1.7 million were in Medicaid - 4.4 million were in separate programs 34.0 32.3 30.8 27.2 25.2 23.5 22.3 21.0 Source: Georgetown Center for Children and Families and CRS. Based on children ever-enrolled over the course of a year.
Trends in the Uninsured Rate of Low-Income Children, 1997 - 2005 Source: Georgetown CCF analysis based on data from the National Health Interview Survey, August 2006. Beginning in 2004, the NHIS changed its methodology for counting the uninsured. This results in the data for 2004 and later years not being directly comparable to the data for 1997 – 2003.
Evidence on Access • Widespread Evidence on Improved Access • Use of preventive care, care for unmet needs, and access to providers increased compared to 6 months prior to enrollment in SCHIP • Racial differences in access, unmet need, and continuity of care appear to be reduced • Improvements in access for children with chronic illness, including asthma Sources: Woolridge et al. (2005). Congressionally Mandated Evaluation of the State Children’s Health Insurance Program: Final Report to Congress. Washington, DC: Mathematica Policy Research, Urban institute; Shone et al. (2005). “Reduction in Racial and Ethnic Disparities After Enrollment in the State Children’s Health Insurance Program,” Pediatrics 115: 697-705; Dick et al. (2004). “SCHIP’s Impact in Three States: How Do the Most Vulnerable Children Fare?” Health Affairs 23(5): 63-75.
Evidence on Other Outcomes • Evidence on Quality • Most states are using quality measures for pediatric preventive and primary care • Evidence on Satisfaction • Over 85% of families of disenrolled children would have kept their children in the program if possible • Evidence on Improved Health • Attacks, urgent health care visits, and asthma-related hospitalizations were reduced for children joining SCHIP Sources: Smith et al. (2006). Quality Performance Measurement in Medicaid and SCHIP: 2006 Survey Results of State Officials. Washington, DC: NACRI; Mitchell et al. (2006). “What Happens to Children Who Lose Public Health Insurance?” Medical Care Research and Review 63(5): 623-35. Szilagyi et al. (2006). “Improved Asthma Care After Enrolling in the State Children’s Health Insurance Program in New York,” Pediatrics 117: 486-96.
ISSUES FOR 2007What is Covered • Benefits • “Too rigid”: States desire for flexibility for “wraps”, etc. • “Too loose”: Concerns about “Secretary-approved” coverage, cost sharing • Quality of Care • Premium Assistance
Who is Covered • Enroll already eligible children • Outreach incentives and options • Parents versus “core” populations • Add excluded low-income children • State employee children, legal immigrant • “Choice” for Medicaid children • Include higher-income children • Option • Parental “mandates” to insure all children
Financing: Budget Challenge Federal Funds Needed to Maintain SCHIP Coverage (FY, Dollars Billions) Estimated Number of Children Losing Coverage: 2.1 Million Source: Broaddus and Park, 2006; assumes moderate expenditure growth.
Distributional Challenge SCHIP Spending as Percent of Allotments, FY 2005 Only 9 States Had Allotments Within +/– 10% of Spending RI Source: C. Peterson, SCHIP Original Allotments: Funding Formula Issues and Options (Washington, D.C.: Congressional Research Service, 2006).
Funding Options • “More Perfect Block-Grant” • Quicker redistribution • Modified allocation formula • Changes in Current Structure • Adjust for actual enrollment • Lift Allotments • Blend matching rates
Reasons for Optimism in Meeting the Challenges • Overall assessment: SCHIP has been a success • Recognition of the value of coverage beyond federal budget costs • Special role that children have in our nation