Download
1 / 34
340 likes | 357 Views
Explore the intricate mechanisms of pulmonary circulation, from anatomy to hemodynamics and thromboembolic disease. Learn about pulmonary hypertension causes and effects. Delve into splanchnic circulation and intestinal physiology. Unravel mesenteric ischemia and its impact on intestinal mucosa.

E N D
Pathophysiologyof Pulmonary and Visceral Circulation Tatár M.
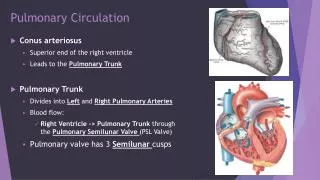
Anatomy • arteries > 1 mm: thin wall, media consists mainly from elastin and collagen fibres • arteries 0.1- 1 mm: muscular layer represents 5% of external diameter • arteriols<0.1 mm: mainly elastic tissue; connections with capillary system, postcapillaryvenules and bronchial arteries (aroundtheneck of terminalbronchioles) • venules: communication with bronchial circulation • veins: media rich of muscle cells – active contraction • bronchopulmonal anastomosis: 2/3 of bronchialblood flows to left atrium
Hemodynamics • high flow with low resistance; enormous blood volume changes without marked pressure changes • pulmonary blood flow depends on respiratory movements and activity of left ventricle • marked effect of left atrium pressure • inspiration improves blood flow into thoracic cavity, expiration improves pulmonary blood flow • main goal of the regulation of pulmonary circulation is to maintaine optimal gas exchange - ventilation is regulated mainly centrally - pulmonary perfusion locally: humoral substances and respiratory gases • mean pressure in pulmonary artery – 12-16 mmHg; in pulmonary veins – 6-10 mmHg
Mechanisms • block of pulmonaryartery (P.A.) flowwithembolus • alwaysassociatedwithdilation of bronchialcirculation • hemorrhagicinfarctionisrelativelyuncommon (bronchialarterysupply) • classification: a) acuteminor b) acutemassive c) subacutemassive d) chronicthromboembolichypertension
Effects on the lungs • smallemboli – no detectableeffect • symptomatology: dyspnea, chestpain • lunginfarction – syptomsarisingfromthecombination of disturbedlungfunction and toxiceffect of feverwithtachycardia and tachypnea Hypoxemiawithnormo- or hypocapnia: - overperfusion of unembolisedlung - ventilation of deadspace - hyperventilation(anxiety)
Effects on the heart and circulation • normalcardiac output evenwhenembolusaffectspulm. function • obstruction of 50% of pulm. circulationiscompromisingrightventricle • sudden and severe obstruction – acuterightventriclefailure(hypotension, dizzeness, syncope), couldprogress to obstructiveshock • subacutemassiveobstructionduringweeks – timeforsomehypertrophy of rightventricle – P.A. pressure 60-90 mm Hg • chronicthromboembolicpulmonaryhypertension– generalizedintimal and medialhypertrophy – chronicrightheartfailure
Causes 1. Idiopathic (primary) PH - arteriopathyofunknownetiology - allbranches of P.A.: medialhypertrophy, fibrinoidnecrosis, narrowing of lumen 2. Heartdiseases a) P.A. bloodflow (left-to-rightshunt) b) pulmonaryvenouspressure (leftheartfailure) 3. Respiratorysystemdisorders (frequently COPD) - alveolarhypoxia(functionalobstruction) a) smoothmusclecontraction in P.A. through a directeffect on intracellularcalcium level b) reduction in NO production - musclehypertrophy in themedia(fixedmorphologicalobstruction) - lossofcapillarybedin areasof severe emphysema
Characteristics of splanchnic circulation • richcollateralsupplyin thisteritory – occlusions a. mesentericainf. result in comparativelylittledisturbances in bloodsupply • portalvenoussystemis of largecapacity and canpool a considerableproportion of bloodvolume • musclevascularplexus in intestinalwallhas more collateralcirculationthanmucosalplexus – in certaintypes of ischemiamucosa has selectivelyundergonecompletenecrosis
Physiology of intestinal circulation • autoregulation: - constantflowwithpressuresbetween 80-160 mmHg to keephydrostaticpressure - precapillaryarterioles in villouscirculationare responsible • postprandialhyperemia • intestinalcounter-currentexchangerforoxygenisinvolvedduringhypotension ischemia of apical part of villoussystem
Mesenteric ischemia • occlusive (embolisation, massivevenoustrombosis): - rare in comparisonwithnon-occlusiveform - transmuralinfarction - loss of circulatingvolume; peritonitis • non-occlusive and relative: - common in criticallyillpatients - cardiacfailure, hypovolemicshock, sepsis
Mesenteric circulation • GIT: - barrieragainstverynoxiousintraluminalenvironment - nutrientsprovideoptimalconditionsforthegrow of microorganisms and helmints • mucosalcirculation: - essentialto sustainebalancebetweenagressiveintraluminal toxins and barriercomponents - compensatoryadjustments in capillarysurficearea and oxygenextraction
Ischemic injury to intestinal mucosa • Hypoxia: • critical level of bloodflow intracellularenergystores • amplification of apicalvillousischemiawithcounter-currentexchange of O2 • intracellularaccumulation of hypoxantine
Ischemic Injury to Intestinal Mucosa 2. Postischemicreperfusion: • freeoxygenradicals • activation of residentneutrophils – anothersource of reactiveoxygenmetabolites • promotion of conversion of xantinedehydrogenase to xantineoxidaseviaproteolysis • proteases (pancreas, granulocytes)
Systemic Mediators of Splanchnic Origin • ischemicbowelreleasestoxicagentswhich, in turn, affectthecardiovascularsystem and lead to development of shock and multiple organ failure • bacterialtranslocation (bacterialleavetheintestinallumen): role of macrophages, ischemicchanges of intestinalarchitecture • endotoxins: Tr and Leu aggregation, abnormaltissueperfusion, capillarypermeability
Syndromes related to splanchnic ischemic injury • stressulceration: acutenon-occlusiveischemicerosions • ischemichepatitis: centrilobularhepatocellularnecrosis • ischemicpancreatitis: due to circulatorydisorderswithoutotherpredisposingfactors • acuteintestinalischemia: severe abdominalpain and intenseperistalticactivity • focalischemia of thesmallintestine: edema, cellinfiltrationintothemucosafollowed by fibrousstricture • ischemiccolitis: damage of mucosal and muscularlayersreplaced by scar and stricture • chronicintestinalischemia (intestinalangina): painoccuring in relation to meals; inability to producepostprandialhyperemia
Ischemic gut as the „motor“ of multiorgan failure • alterations in gutadynamicileus, „thirdspace“, hypermetabolism, loss of barrierfunction - uppergutiscolonised by pharyngealmicroflora - aspirationpneumonia = invasion of gastricflora • source of endogenousvasodilators in hemorrhage, cardiacfailure, sepsis - damage of mucosalbarrierbacterialtranslocation toxinsintothecirculation