Download
1 / 15
170 likes | 446 Views
Skull Deformities in Pediatrics. Case 1. 7wk female with parental concern over head shape PMHx: 35wk twin A; NICU x 6days (FEN, ID, bili) Normal feeding/wets/stools Progressive “flattening” of head since birth No hx IVH; no neurological symptoms No flattening in twin. Case 1.

E N D
Case 1 • 7wk female with parental concern over head shape • PMHx: • 35wk twin A; NICU x 6days (FEN, ID, bili) • Normal feeding/wets/stools • Progressive “flattening” of head since birth • No hx IVH; no neurological symptoms • No flattening in twin
Case 1 • Physical Exam: • Ht, Wt, HC tracking • Alert, NAD • AFOSF, RR present • Flattened R occiput, with protrusion of R forehead and R ear farther forward • Mild flattening of L face • O/W unremarkable
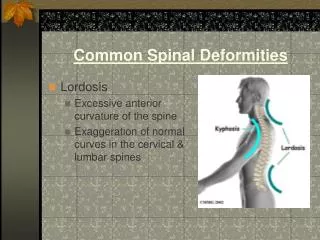
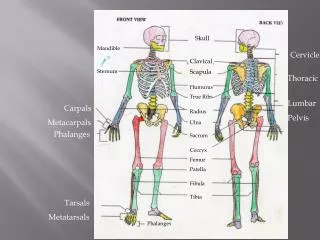
What’s normal? • Skull growth mainly secondary to brain growth • 40% adult size at term • 90% adult size by 1yo • 95% adult size by 6yo • Suture closure • PF 3-6mo • AF 9-18mo • C,S,L sutures 40years
What’s most likely? • Deformational Plagiocephaly: • Asymmetric head • Up to 48% healthy infants • Most common referral to Peds NSGY • Risk Factors: • Intrauterine crowding/positioning • Decreased mobility (dev.delay, MR, prematurity) • Posturing (torticollis, C-spine defect) • “Back to Sleep” campaign • Increased physician awareness
What’s the worry? • Craniosynostosis: • Premature closure of sutures • 1 in 2,100-3,000 live births • Isolated (80%) vs. Syndromic (20%) • Risk Factors: • Single-gene mutations (FGFR, TWIST, MSX2) • Rickets, hyperthyroidism • Phenytoin, retinoids, VA, MTX, fluconazole
What’s a Pediatrician to do?The H&P, of course! • Molding • Pressure in AP dimension (labor) • Resolves in hours-weeks • Deformation • Pressure in local region (occipital) • No sutural ridging; bones mobile • Synostosis • Premature closure of sutures • Palpable ridges over suture; bones immobile
What’s normal? PARALLELOGRAM TRAPEZOID Deformational Plagiocephaly Lambdoid Synostosis
What’s not? Metopic Synostosis Bicoronal Synostosis
What’s not? Sagittal Synostosis
Deformational Plagiocephaly • AKA: Positional, Posterior, Occipital, Plagiocephaly without synostosis • Diagnosis: • Usually clear based on H&P • Head shape (parallelogram) • Xray if unsure – sutures patent
Deformational Plagiocephaly • Treatment: • Repositioning • Effective in 85% mild cases • Alternate sleeping sides • Encourage “tummy time” • Discourage carseats • Helmet • 23 hrs/day • Frequent adjustments • Typically does not require NSGY referral
When to refer? • True craniosynostosis • 1/5-1/6 syndromic • Increased risk ICP, hydrocephalus, Chiari • Multi-D Team: • NSGY, Plastics, Ophtho, Neuro, ENT, Orthodontics, Psych, Genetics, Social Work • Neurosurgery: 3-9 months old
Case 2 • Newborn female, term SVD • No maternal hx; no family hx • Physical Exam: • Large, low AF • ?Fused coronal/lambdoid sutures? • Significant caput • Hypertelorism • Syndactyly on 3 extremities; clubfoot • Broad, flat hallux
Case 2 • Craniofrontonasal Dysostosis • X-linked • Variable expression (F>M) • Genetics eval • Orthopaedics eval • Ophthalmology eval • Neurosurgery/OMFS eval