Download
1 / 44
550 likes | 1.14k Views
Weaning from mechanical ventilation in 21 st century. Dr P K Dash SCTIMST, Trivandrum. Aim of ventilatory care. Goals of mechanical ventilation. Discontinuing ventilation . Initiating ventilation . Easy Quick May not be controversial. Difficult Time consuming Controversial.

E N D
Weaning from mechanicalventilation in 21st century Dr P K Dash SCTIMST, Trivandrum
Discontinuing ventilation Initiating ventilation • Easy • Quick • May not be controversial • Difficult • Time consuming • Controversial
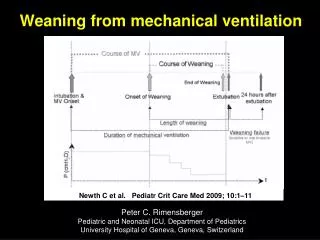
Do Not Wait Weaning from ventilation vs Discontinuation of ventilation
Most accepted method • Spontaneous breathing trials • T Piece • Pressure Support • CPAP
Most commonly used • Partial ventilatory support • SIMV • SIMV with PS • Less Tried • NIV • BIPAP
Evolution of Modes • Volume control • Pressure control • Pressure support • Dual control • Algorithm based • Knowledge based
Knowledge based weaning 2005 1994 2006 1992
Smart care • It is a knowledge based automated weaning system. • It contains an automated clinical weaning guideline • Based on recognised medical expertise and research.
Preconditions • patient body weight 35-200 kg • ventilator in adult mode • CPAP/ASB mode • automatic tube compensation deactivated • invasive ventilation via ETT or tracheostomy • apnoea ventilation on and properly set • end tidal CO2 monitoring through the ventilator • flow monitoring activated • ΔPASB should be between ΔPASB goal+5 and 35 • PEEP 0-20
Smart Care • Zone of Respiratory Comfort • Spontaneous breathing frequency (fspn) 15-30 cycles/min, • up to 34 in patients with neurologic disease • Spontaneous tidal volume (VT) Vt > 300 ml • 250 if weight < 55 Kg, • Endtidal CO2 (etCO2)PetCO2< 55mmHg • 65mmHg if COPD
Smart care working principle • Step 1: Stabilizing within a respiratory comfort zone • Step 2: Reducing invasiveness • Step 3: Testing readiness for extubation
Trigger point Ideal Technology Central Nervous System Phrenic Nerve Diaphragm Excitation Diaphragm Contraction Chest Wall and Lung Expansion Airway Pressure, Flow and Volume New Technology Ventilator Unit Neuro-Ventilatory Coupling Current Technology
Conventional triggering Conventional ventilator technology uses a pressure drop or flow reversal to provide assistance to the patient. This is the last step of the signal chain leading to inhalation. This last step is subject to disturbances such as intrinsic PEEP, hyperinflation and leakage.
Nava triggering • The earliest signal that can be registered with a low degree of invasivity is the excitation of the diaphragm. • The excitation of the diaphragm is independent of pneumatic influence and insensitive to the problems with pneumatic triggering technologies. • By following diaphragm excitation and adjusting the support level in synchrony with the rise and fall of the electrical discharge, the ventilator and the diaphragm will work with the same signal input. • In effect, this allows the ventilator to function as an extra muscle, unloading extra respiratory work induced by the disease process.
Signal capture • All muscles (including the diaphragm and other respiratory muscles) generate electrical activity to excite muscle contraction. • The electrical activity of the diaphragm is captured by an esophageal catheter with an attached electrode array. The signal is filtered in several steps and provide the input for control of the respiratory assist delivered by the ventilator.
Catheter verification • P and QRS waves are present on the top leads and the P-waves disappear on the lower leads and with a decrease of the QRS-amplitude on the lower leads. • When an Edi waveform is present, observe which leads are highlighted in blue. If the leads highlighted in blue are in the center (i.e. second and third leads), secure the Edi Catheter in this position. • To finally verify correct positioning of the Edi Catheter press the Exp. Hold and keep the button depressed until a breathing effort is registered. A negative deflection in the pressure curve with a simultaneous positive inflection in the Edi curve verifies correct position of the Edi Catheter.
Setting the NAVA level NAVA preview is a help tool to set the NAVA level to reach an estimated NAVA On the uppermost waveform (the pressure curve), there are two curves presented simultaneously. The gray curve shows the estimated pressure, Pest, based on the Edi signal and the set NAVA level. NAVA preview is available in all invasive modes of ventilation except NAVA.
Reintubation and Steroids A reintubation rate of 10% is acceptable. Patients deserve a trial of extubation, and many will do well in spite of poor mechanics A high-risk population to develop post-extubationstridor and reintubation can be identified by a cuff-leak test (a low level of leak less than 110 ml or less than 25%). There is convincing evidence for giving steroid therapy at least four hours before extubation to prevent stridor and reintubation in a high-risk population. The steroid benefit remains unclear when patients are not selected.