Download
1 / 37
380 likes | 723 Views
Acid-base Balance and its Disorders. Prof. Dr. Meltem Pekpak. For optimal functioning of cells. Acids and bases in the body must be in balance. We all consume every day food and drinks which contain acids, metabolism produces also acids. Body pH Balance. Chemical blood buffers: Lungs,

E N D
Acid-base Balance and its Disorders Prof. Dr. Meltem Pekpak
For optimal functioning of cells.. • Acids and bases in the body must be in balance. • We all consume every day food and drinks which contain acids, metabolism produces also acids...
Body pH Balance • Chemical blood buffers: • Lungs, • Cells, • Kidneys • Defences against changes in hydrogen concentration (getting acidotic..)
You get acidotic every day ! • While living, eating and drinking...there is.. • Production of 1 mmol of fixed acid/kg body weight per day (60 kg=60 mmol/day)
Buffers • Extracellular: • Hemoglobin • (‘Chloride shift’-for each chloride leaving the cell-one bicarbonate ion enters) • Plasma protein • (with the liver, varying the amount of H-ions in the protein structure) • Bicarbonate system: • Normal acid to base ratio is 20:1 • 20 parts bicarbonate to 1 part carbonic acid (H2CO3=CO2), • Neutralizing a strong acid bicarb. will be lost
Human Acid-baseHomeostasis • Tight regulation: • CO2 tension • by respiratory excretion (of volatile acids) • Plasma bicarbonate [HCO3-] • By renal HCO3- reabsorption and • Elimination of protons produced by metabolism • pH is determined by CO2 tension and [HCO3-]
Physiology of Buffering: • Ability of a solution containing a weak or poorly dissociated acid and its anion (a base) to resist change in pH when strong acid or alkali is added • 1 ml of 0.1 M HCl to 9 ml distilled water = • [H+]from 10 -7 M to 10 -2 M= pH from 7 to 2 • 1 ml of 0.1 M HCl to 9 ml of phosphate buffer: dissoc. H+combines with [HPO42-] = (H2PO4-) • pH fall of only 0.1= to 6.9
Bicarbonate Buffer • Extracellular most important buffer • Proteins and phosphate buffer less important • Intracellularphosphate- most important b. • Equilibrium conditions because abundant carbonic anhydrase in blood • H+ + HCO3- H2CO3 H2O + CO2 • [H+ ]= Keq x [H2CO3 ]/[HCO3-]
Equations • H+ + HCO3- H2CO3 H2O + CO2 • Equilibrium • [H+ ]= Keq x [H2CO3 ]/[HCO3-]
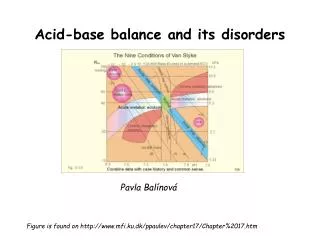
Total Acid- base Metabolism Henderson-Hasselbalch 1909,1916 Altered by Buffering Primarily Altered in Metabolic Disorders HCO3- • pH = pK + log ------------ PaCO2 Metabolic comp. Respiratory component Primary Respiratory Disorders Altered by Respiratory Compensation for Metabolic Disorders Result of Metabolic and Respiratory Interplay
Normal Values • [HCO3-] ~ 24 mM • PaCO2 = 38 torr • pH ~ 7.42 • Plasma HCO3- regulation by • reclaiming filtered HCO3- and • generating new HCO3- (carboanhydrase) • ( to replace the lost internally titrating metabolic acid and externally from the GI tract) • Production of 1 mmol of acid/kg body weight per day (60 kg=60 mmol/day)
Renal Acid -base Handling • Two seperate functions: • Bicarbonate reabsorption • Net acid secretion
Proximal Tubular BicarbonateReclamation Process (90 %) Two vehicles for apical H+ secretion (Na+/H+ exchanger), H+ATPase. Basolateral ion pumps: Na+/K+ ATPase, (Na+HCO3-)symporter,HCO3-/Cl- Exchanger. The role of carbonic anhydrase (CA) in tubular cell and brush border
Net Acid Excretion • Urine is acid = pH~ 4.5 • Buffer salts are in the tubular fluid • Phosphate is the most important buffer in urine: HPO42- + H+ = H2PO4- • Nonvolatile (fixed) acids (anions= sulfates, phosphates) must be accompanied in the urine by equivalent cations (Na +, K +, Ca + +) for maintenance of electrical neutrality • In acid urine ammonium helps to keep [H+ ] (ammonia NH3+ to NH4+)
Clinical Evaluation • Patient history • Clinical presentation • Acidemia Hyperventilation • Alkalemia Paresthesias and Tetany • Laboratory: Blood acid-base status: • Blood pH (4 º C, with anticoagulant, promptly), • Urine pH • Plasma and urine electrolyte concentration • Lactate concentration
Acidosis • Clinical effects of severe acidosis: pH <7.2 • Cardiovascular system effects: • Decreased myocardial contractility • Decreased cardiac output • Cardiac failure • Hypotension • Decreased hepatic and renal blood flow • Centralization of effective blood volume • Tissue hypoxia • Pulmonary edema
Metabolic acidosis • Hallmark is [HCO3-] • 1. Acid production net acid intake above net renal excretion (ketoacidosis, lactic acidosis, ammonium chloride loading) • 2. failure of renal net excretion (chronic renal failure, renal tubular acidosis) • 3. Bicarbonate loss via the gastroinestinal tract (diarrhea, gastrointestinal fistula) • 4. Nonbicarbonate solutions added to ECF (dilutional acidosis)
Steps of evaluation • 1.Examine pH= Reduction ( 7.2) Acidosis • Increase (7.5) Alkalosis • 2. Examine directional change of PCO2 • and [HCO3-] , • pH acid, HCO3- low Metabolic acidosis • pH alkal., HCO3- high Metabolic alkalosis • 3. Assess degree of compensation: Mixed acid-base disorder? • Metabolic acidosis PCO2 • Metabolic alkalosis PCO2 • Failure of respiratory compenstion= primary respiratory acid-base disorder • Never to initial pH through compensation !!
Steps of evaluation • 4. Calculate the serum anion gap • Is the acid-base disorder organic or mineral in origin?? • We use venous sample blood electrolytes: • Electroneutrality demands: • Serum anion gap, that means: • [Na+] + [UC]= [Cl-] +[Total CO2] + [UA] • (U means: unmeasured)
Normally the serum anion gap is about 9 (6-12 mEq/l), a major increase in Anion gap > 26 mEq/l always implies existence of an organic acidosis
Differential Diagnosis of Metabolic Acidosis • Normal anion gap Increased anion gap • (hyperchloemic) (organic)_________ • GI loss ofHCO3- acid production • Diarrhea Lactic acidosis • Renal tub. Acidosis Diab. Ketoacidosis • Parenteral alimentation Toxic alcohol,salicy. • Carbonic anhydr. İnh. Acute renal failure • K-sparing diuretics Chronic renal failure
Increased anion gap Metabolic acidosis • Ketoacidosis (diabetic) • Uremia (renal failure) • Salicylate intoxication • Starvation • Methanol intoxication • Alcohol ketoacidosis • Unmeasured osmoles (intoxication) • Lactic acidosis
Simple decompensatedAcid-base Disorders • Acid Base Dis.: pH pCO2 HCO3- • Metabolic acidosis • Respiratory acidosis • Metabolic alkalosis • Respiratory alkalosis
Compensatory Response one half of acid load is buffered by nonbicarbonate buffers= Bone, protein, red cells.. • PCO2 (Kussmaul) • compensatory response after 15-30 minutes, • 5 days up to maximal • Kidney: • Metabolic acidosis • processing of glutamine into NH4+ (ammonia to ammonium for better H-excretion) and • Bicarbonate generation (and reclaiming)
Respiratory Acidosis • Acute increase in pCO2 • Buffered primarily by intracellular buffers • Chronic state: • Kidneys compensation: • Increase net acid excretion, • (48 hours for fully development) • Underlying cause: • Central nervous system disease, • lung (COPD)and heart disease, • sedatives and opiates depressing the respiratory center • Hypercapnic encephalopathy can develop
Metabolic Alkalosis • Plasma bicarbonate [HCO3-] = pH • 1) H+ GI loss or shift into cells • 2) Excess HCO3- Administration of bicarbonate, or precursors: lactate, acetate, citrate or Failure to excrete: mineralocorticoid effect • 3) Loss of fluid with Diuretic therapy [Cl-], [K+] and [H+] loss from plasma- extracellular volume contraction
Volume Depletion and Metabolic Alkalosis • Absolute volume depletion: • Loss of salt by bleeding or vomitting or • Effective volume depletion: • Heart failure, cirrhosis, nephrotic syndrome whenever • GFR • Tubular HCO3- reabsorption • Because proximal tubule reabsorption is enhanced for Na and water
Compensatory Respiratory Response • Alveolar hypoventilation(hypercapnia) • (limited pCO2riseto 50-60 mm Hg) • Kidneys: • Excretion of HCO3-proportional to GFR (excessive)
Respiratory Alkalosis pCO2 , pH due to: Hypoxia (compensatory hyperventilation) • Acute: pulmonary edema or emboli, pneumonia, • Chronic: severe anemia, high altitude, hypotension Respiratory center stimulation • Pregnancy, Anxiety, Fever, heat stroke, sepsis, salisylate intox., cerebral disease, hepatic cirrhosis, Increased mechanical ventilation
Respiratory Alkalosis • Most common acid-base disorder • Physiologic in pregnancy and high altitude • Bad prognosisin critically ill patients (the higher hypocapnia, the higher mortality) • Hyperventilation, • Perioral and extremity paresthesias, • Light-headedness, • Muscle cramps, • Hyperreflexia, seizures, ionized Ca tetany
Metabolic Alkalosiswith and without Volume Depletion • Volume depleted- Chloride responsive metabolic acidosis: • Urine chloride is low (<10 mmol/l) • Due to: • Gastric fluid losses • Stool losses • Diuretic therapy
Metabolic AlkalosisExcessive Mineralocorticoids • Mineralocorticoidsstimulatehydrogenionsecretion • And thisbicarbonate reabsorption • Urinary chloride is normal (<20 mmol/l) • Hypokalemia • Primary aldosteronizm, • Bartter’s Syndrome, • Cushing Syndrome • Renovascular hypertension
Proximal Tubular Bicarbonate Reclamation Process (90 %) The proximal tubulus cells form carbonic acid from carbon dioxide and water under the influence of the enzyme carboanhydrase (CA). Carbonic acid ionizes to yield hydrogen and bicarbonate . Hydrogen formed in the cell exchanges with sodium in the tubular fluid (dashed circle). As a net effect Sodium bicarbonate is reabsorbed, and the hydrogen ion secreted into the tubular lumen is buffered by filtered bicarbonate.
Henderson-Hasselbach 1909,1916 • H2CO3 = p CO2 +solubility in physiol. Fluids • [H+ ]= K x [S x pCO2 ]/[HCO3-] Antilog of both sides: pH= pK + log10 [HCO3-] / [S x PCO2] In blood at 37º C, pK =6.1 and S is 0.03 pH= 6.1+ log10 [HCO3-] / [0.03 x PaCO2]