Download
1 / 57
570 likes | 691 Views
CRS. Center for Resuscitation Science. SHOCK! Focusing on ED and sepsis. David F. Gaieski, MD Assistant Professor, Department of Emergency Medicine Clinical Director, Center for Resuscitation Science University of Pennsylvania School of Medicine gaieskid@uphs.upenn.edu. Critical Care.

E N D
CRS Center for Resuscitation Science SHOCK!Focusing on ED and sepsis David F. Gaieski, MD Assistant Professor, Department of Emergency Medicine Clinical Director, Center for Resuscitation Science University of Pennsylvania School of Medicine gaieskid@uphs.upenn.edu
Critical Care • Critical care is a concept not a location • It is a way of treating patients that begins in the pre-hospital setting with EMS care, continues in the ED, and is completed in the ICU Safar P. Critical care medicine---quo vadis? CCM. 1974;2:1-5.
Outline • Definition of shock • Oxygen delivery • Etiology of shock • Septic shock • Goal-directed resuscitation • The importance of antibiotics
What is Shock? • Heart rate > 150 • Inadequate carbon dioxide clearance • Systolic Blood Pressure < 100 • Physiologic state characterized by inadequate oxygen delivery
What is Sepsis? • Infection plus shock • Infection plus positive culture source • Infection plus hypotension • Infection plus inflammation
Central Venous Pressure is a surrogate for: • Preload • Afterload • Contractility • Venous oxygen saturation
Which of the following does not directly effect oxygen delivery? • Hemoglobin • Lactate • Cardiac output • Arterial oxygen saturation
“I’m all congested up here” • 53 y/o African American Male • HPI • 1 week chest congestion, cough, f/c • PMH • Seizures, thrombocytopenia • SH • Heavy EtOH, 1 ppd tobacco
Temp: 101.6° F BP: 97/65 HR: 135 SpO2: 86% on RA RR: 32 Triage Vital Signs
Physical Exam Gen: WDWN male in respiratory distress HEENT: Sclerae icteric; MM dry Lungs: Decreased BS at left base, dullness to percussion; rhonchi R mid lung field CVS: Tachy nml S1, S2; - obvious murmur ABD: NT, ND, + BS EXT: - C, C, E Skin: No rash, hot to touch Neuro: Alert, but fatigued
Initial Management IV access Supplemental oxygen Cardiac monitoring Fluid resuscitation Labs, cultures, CXR Antibiotics Is this patient in shock?
What is Shock? • First clinical definition in the1800s by John Collins Warren “A momentary pause in the act of death” • Warren JC. Surgical pathology and therapeutics. Philadelphia: 1895. • 1872 - Samuel Gross “A rude unhinging of the machinery of life” • Gross SG. System of surgery: Pathological diagnostic, therapeutique, and operative. Philadelphia: Lea & Febiger; 1872
What is Shock? • A physiologic state characterized by • Inadequate oxygen delivery • Delivery isn’t keeping up with demand • Oxygen Delivery
Oxygen Delivery Oxygen Delivery Oxygen Consumption Venous Oxygen Saturation = HR x SV CO x CaO2 = (SaO2 x Hgb + (0.0031 x PaO2) x 1.34)
DO2 Consumption (VO2) Delivery independent VO2 Delivery dependent
The 3 Causes of Shock Volume Resistance Pump Some types have > 1 cause
Inadequate volume • Problem: Decreased Preload • ↓preload ↓SV ↓CO ↓DO2 • Causes • Absolute • Hemorrhage, dehydration • Relative • Vascular leak, increased v. capacitance • Treatment • Volume
Inadequate resistance • Problem: Inappropriate ↓SVR • Multiple causes • SIRS Inflammatory cascade • Pancreatitis, burns, trauma, sepsis • Anaphylaxis • Addisonian crisis • Treatment • Vasopressors
Pump failure • Problem: Contractility or HR • ↓SV or ↓HR ↓CO ↓DO2 • Multiple causes • Acute MI, arrhythmias, tox, sepsis • Treatment • Inotropes/chronotropes • Electricity • Cardioversion • Pacing
Hemodynamic Response to Hemorrhage % of Control Vascular Resistance 100 Blood Pressure Cardiac Output 25% 50% % Plasma Loss
Cryptic Shock • SBP > 90 or MAP > 65 • Profound tissue hypoxia • Associated with elevated lactate
831/856 (97%) of admitted severe sepsis pts had lactate sent Median lactate=2.9 mmol/L 28 day mortality: 22.7% Divided into: Low: ≤ 2mmol/L Medium: > 2 to ≤ 3.9mmol/L High: ≥ 4mmol/L Stratified to presence or absence of refractory hypotension Mikkelsen ME et al. Crit Care Med, 2009
ED Lactate in Severe Sepsis Mortality (%) Lactate (mmol/L) Mikkelsen M, et al. CCM. 2009
ED Lactate in Severe Sepsis Mortality (%) Lactate (mmol/L) Mikkelsen M, et al. CCM. 2009
“Except on few occasions, the patient appears to die from the body’s response to infection rather than from…[the infection itself….]” - Sir William Osler, 1904
The Continuum of Sepsis SIRS Sepsis Severe Sepsis Septic Shock • Systemic Inflammatory Response Syndrome • SIRS criteria • Temp < 96.8° or > 100.4° F • HR > 90 • RR > 20 or PCO2 < 32 • WBC < 4 or > 12 or bands > 10% Bone et al. Chest 1992;101:1644
The Continuum of Sepsis SIRS Sepsis Severe Sepsis Septic Shock • Systemic Inflammatory Response to Infection • Suspected or confirmed infection • 2 or more SIRS criteria Bone et al. Chest 1992;101:1644
The Continuum of Sepsis SIRS Sepsis Severe Sepsis Septic Shock • Sepsis plus Organ Dysfunction • Elevated Creatinine • Elevated INR • Altered Mental Status • Elevated Lactate • Hypotension that responds to fluid Bone et al. Chest 1992;101:1644
The Continuum of Sepsis SIRS Sepsis Severe Sepsis Septic Shock • Cryptic Shock • Normotensive • Lactate > 4 • Severe Sepsis and Hypotension • Hypotension that does NOT respond to fluid (30 cc/kg bolus) Bone et al. Chest 1992;101:1644
Mortality in Admitted Patients Mortality, % RANGEL-FRAUSTOJAMA1995
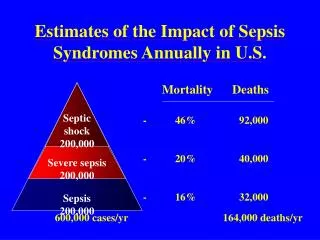
Why is this so Important? • 750,000 cases/yr of severe sepsis in US • 215,000 deaths/yr directly related to sepsis • Tenth leading cause of death in USA • Rate of sepsis cases is increasing faster than the population • 37% of severe sepsis patients come through the ED Angus DC, et al. Crit Care Med, 2001
EGDT • Design • Randomized, controlled trial • Patients • 263 adults with severe sepsis and lactate > 4 or septic shock • Intervention • 6 hours of algorithmic care which optimized • CVP 8-12 • MAP > 65 • ScvO2> 70% • Outcome variables • Mortality in-house, 28 day, and 60 day
ScvO2 stratified into 3 groups: • Hypoxia: ScvO2 < 70% • Normoxia: 70-90% • Hyperoxia: > 90% • Examined initial and maximum ScvO2 during ED course • Primary outcome: IHM
Results Maximum ScvO2 achieved in ED
Schemata for classification of oxygen supply and utilization
EGDT Survival Rivers E. N Engl J Med 2001:345:1369-77.
CVP ≥8 Yes No Bolus 500 ml NS q15-20 MAP ≥ 65 baseline No Yes 1. Start/Titrate norepi or dopamine 2. Dexamethasone for refractory hypotension 3. Place arterial line if time permits ScvO2≥ 70% Yes No Transfuse PRBC’s until HgB ≥ 10 ScvO2≥ 70% Yes No Start/Titrate Dobutamine ScvO2≥ 70% Yes No CVP, MAP, ScvO2 goals achieved Re-evaluate to achieve goals
How’s Our Patient Doing? • SpO2 91%, RR 36, HR 130, BP 138/74 • Notable labs: • WBC: 5.3 • Hgb: 15 (Hct - 43) • Platelet: 19 • BMP 131/3.5/94/16/23/2.0/116 • INR – 1.8, PTT – 46.2 • Tbili=6.6; direct=5.3 • Lactate 8.4 • CXR: Right Lower Lobe pneumonia Cryptic Shock
ED Course • Cefepime/Azithromycin • Intubated for hypoxemia, AMS, ↓ WOB • ScvO2 catheter placed • Arterial line placed • Initial ABG – on 100% FiO2 • 7.27/42/126/-6.6 P:F ratio = 126
ED Course • CVP – 8 (intubated) • 500 cc NS bolus q 30 min until CVP – 12 • Total intake – 9L • MAP • Initially 70s, dropped to 60 • Norepinephrine started at 1 mcg/min • Maintained MAP >65 with norepi @ 2 • ScvO2 • Remained 70-80%
ED Course • Repeat Labs • Creatinine – 1.1 (2.0) • Lactate – 5.8 (8.4) • Base Deficit – 1.0 (6.6) • pH – 7.38 (7.27) • Transferred to MICU • Continued Goal-Directed Therapy
Case Conclusion • Blood and Sputum Cx • Streptococcus pneumoniae • Weaned off vasopressors HD # 5 • Self-extubated at HD # 5 • D/c’ed home on hospital day # 14