Download
1 / 36
380 likes | 1.01k Views
Diabetic Neuropathy. Patrick English Diabetes Consultant Derriford Hospital. Outline. Size and costs of the problem Pathology/pathophysiology Risk factors Presentations Diagnosis Prevention and Treatment Algorithm/NICE. Size and cost. Prevalence: 22.7% T1DM, 32.1% T2DM

E N D
Diabetic Neuropathy Patrick English Diabetes Consultant Derriford Hospital www.plymouthdiabetes.org.uk/
Outline • Size and costs of the problem • Pathology/pathophysiology • Risk factors • Presentations • Diagnosis • Prevention and Treatment • Algorithm/NICE www.plymouthdiabetes.org.uk/
Size and cost • Prevalence: 22.7% T1DM, 32.1% T2DM • USA: 17% of costs of treating diabetic complications (approx $300 per patient per year) • UK: £13 million p.a on diabetic foot complications • 1900 patients with painful diabetic neuropathy in Derriford Catchment • 435 requiring at least 2nd line agent for pain • Young MJ, Boulton AJ, MacLeod AF, Williams DR, Sonksen PH. Diabetologia 1993;36(2):150-4. • Caro, J. J., A. J. Ward, et al. (2002). Diabetes Care25(3): 476-81. www.plymouthdiabetes.org.uk/
Pathology • Axonal loss, focal demyelination & regeneration • conduction velocity and sensory thresholds www.plymouthdiabetes.org.uk/
Pathophysiology-biochemical and vascular factors www.plymouthdiabetes.org.uk/
Risk Factors • Glycaemic control-DCCT • with age: 5% 20-29 years, 44.2% 70-79 years • > 50% T2DM >60 years of age • with duration of diabetes: 20.8% < 5years, 36.8%>10 years • Smoking • Microalbuminuria • Height • ? Nutritional factors www.plymouthdiabetes.org.uk/
Presentations 3 types of neuropathy: • Progress steadily with increasing duration of diabetes and associated with other diabetic complications-common • Acute onset with resolution over period of months-rare • Pressure palsies www.plymouthdiabetes.org.uk/
Presentations Diffuse symmetrical sensorimotor polyneuropathy • Predominantly sensory • Predominantly feet • pain and temperature sensation • Parasthesiae and numbness • Neurogenic pain/allodynia • Neuropathic oedema • Wasting occurs only if severe www.plymouthdiabetes.org.uk/
Diffuse symmetrical sensorimotor polyneuropathy Problems: • Pain and oedema • Diabetic foot ulceration • Present in 80% of foot ulcers • Principle cause in 39% of ulcers • Partly responsible in 36% of ulcers www.plymouthdiabetes.org.uk/
Autonomic Neuropathy • Closely associated with sensorimotor neuropathy • Signs are common if looked for (40% subjects have abnormal CVS tests) but symptoms are rare (<1%) • Affects the response to hypos but not awareness • If symptoms: mortality=30-50% over 10 years www.plymouthdiabetes.org.uk/
Diffuse Small Fibre Neuropathy • T1DM • Young, ♀ > ♂ • Selective damage to small nerve fibres • Pain and temp lost but LT retained • Symptomatic autonomic neuropathy, Charcot arthropathy and foot ulcers • ? autoimmune www.plymouthdiabetes.org.uk/
Mononeuropathies Acute ? Secondary to ischaemia • Pain and weakness (severe) • Resolve over months • Amyotrophy (Older ♂>♀) • 3rd nerve • 6th nerve • Truncal radiculopathies www.plymouthdiabetes.org.uk/
Insulin Neuritis • Acute & diffuse • May be painful • Follows improvement of blood glucose control • ?steal phenomenon www.plymouthdiabetes.org.uk/
Acute diffuse painful neuropathy • Not related to duration of diabetes or complications • Association with marked weight loss • severe burning/shooting pain, “electric shocks”, allodynia • Resolve spontaneously, usually with weight gain, 6-8 months. Some 2 years. • Does not relapse • Signs may be lacking and dissociated from symptoms www.plymouthdiabetes.org.uk/
Pressure Palsies • susceptibility to pressure damage • Limited joint mobility (soft tissue) • Carpal tunnel • Ulnar nerve • Lateral popliteal nerve
Diagnosis Annual review • Enquire annually for: · Painful neuropathy · Loss of sensation · Erectile impotence • Note duration of DM, treatment, complications & weight • Ask about other manifestations of autonomic neuropathy if: · Other complications are present · Anaesthesia is contemplated · Blood glucose control is erratic www.plymouthdiabetes.org.uk/
Diagnosis Examine: • For evidence of peripheral neuropathy annually • LT • OR if new symptoms • Vibration • LT • ?Thermal thresholds • ?Pain • For postural hypotension if symptoms of autonomic neuropathy
Examination-ANS Ewing’s battery Abnormal results common • Valsalva-expiration for 15 secs against 40 mmHg. Rest 1 min then repeatx2. • Avoid in proliferative retinopathy. • RR max : RR min>1.21 =Normal, <1.20 = abnormal. • HR increase on standing • RR 30:15 ratio > 1.04 • HR at max overshoot or 15 seconds 15bpm (abnormal if<12) www.plymouthdiabetes.org.uk/
Ewing’s battery • HR variation during deep breathing (6 breaths per minute) • Max-min > 15bpm (<10 is abnormal) • Postural BP-2 mins after standing • Fall< 10mmHg normal • >30 mmHg abnormal www.plymouthdiabetes.org.uk/
Diagnosis Consider differential diagnoses • HSMN • Ethanol • B12/folate • Malignancy • Renal failure • Drugs • AI disease • Cord problems • Leprosy www.plymouthdiabetes.org.uk/
Prevention Control • DCCT (1995) • Tight control-3% neuropathy at 5 years • Conventional-10% • UKPDS (1998) • Tight control (HbA1c 7%)-31.2% neuropathy at 15 years • Conventional (HbA1c 7.9%)-51.7% • P=0.005 • No protective effect seen for BP control www.plymouthdiabetes.org.uk/
Prevention • Aldose reductase inhibitors • Gamma Linoleic Acid • Vasodilators-ACE? • AGE inhibitors • Antioxidants • NGFs • ? Smoking cessation, ? BP reduction www.plymouthdiabetes.org.uk/
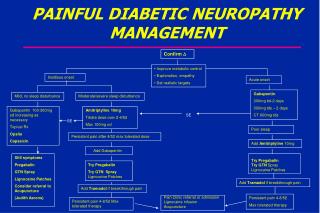
Treatment-Painful neuropathy • General Measures • Improve glycaemic control • Exclude or treat other contributory factors • Alcohol excess • Vitamin B12 deficiency/Folate • Uraemia • Simple analgesia-NSAID/Paracetamol • Explanation, empathy and reassurance Choose drugs according to dominant symptoms • Other symptoms • Allodynia • Plastic film • Leg cradle at night • Restless legs • Ropinirole • Painful Cramps • Quinine sulphate Lancinating pain Tricyclics Anticonvulsants Duloxetine Burning pain Tricyclics Anticonvulsants Duloxetine
NICE CG 87 May 2009
Treatment -ANS Postural hypotension • Fludrocortisone • NSAIDs • Compression stockings • Elevate the head of the bed www.plymouthdiabetes.org.uk/
Treatment -ANS Bladder • Manual SP pressure • ISC • ? Anticholinesterase • Cyclical antibiotics if recurrent infections Sweating • ?clonidine Erectile dysfunction www.plymouthdiabetes.org.uk/
Treatment -ANS Gastroparesis • Improve glycaemic control • Prokinetic drugs • Metoclopramide, domperidone, cisapride, erythromycin (250 mg tds) • Octreotide? • If severeadmit for IV fluids, IV drugs NG tube IV/jejunal feeding Diarrhoea • Codeine/loperamide/diphenoxylate • Clonidine or octreotide • Treat bacterial overgrowth (oxytet/erythromycin) if suspected/present www.plymouthdiabetes.org.uk/
Any questions? • www.plymouthdiabetes.org.uk