Download
1 / 51
510 likes | 624 Views
Adapting to Changes in Medicare 2007. Who should attend. Physician Leader of the Practice President of the PA, Founder Practice Administrator CEO, Executive Director, COO Contracting Officer Contract Administrator, Director of Billing Clinical Manager

E N D
Who should attend • Physician Leader of the Practice • President of the PA, Founder • Practice Administrator • CEO, Executive Director, COO • Contracting Officer • Contract Administrator, Director of Billing • Clinical Manager • Medical Director, Nursing Team Leader
After this session, you will be able to: • Identify changes in Medicare coding and reimbursement for 2007 • Assess the degree to which your practice has made the necessary changes to adapt to new Medicare regulations • Understand the role of the physician practice leader and the administrator in adapting to these changes
Today’s Topics • Medicare Physician Fee Schedule 2007 • Hospital Outpatient Prospective Payment System 2007 • Drug Reimbursement • Part D Update • Oncology Coding Update • ICD-9, CPT, HCPCS • Drug administration coding review • Role of the physician practice leader and administrator • Resources
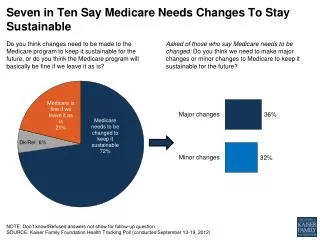
Medicare Physician Fee Schedule 2007 Final rule published 12/1/06 • Annual Update • Final rule reported 5.0% decrease in conversion factor; Congressional action on 12/9 holds CF at 2006 rate ($37.8975) • Practice Expense Relative Values • Methodology revised; four year phase in period • Payment for most drug administration services will decrease slightly • CMS projects 1% decrease in oncology payments when change is fully implemented in 2010
Medicare Physician Fee Schedule 2007 • Physician Work Relative Values • Work relative value increased for many E/M codes, across all specialties • CMS estimates increase in overall payments for oncology, perhaps as much as 3% • Budget neutrality requirement results in 10.06% decrease to physician work relative values for all codes across the fee schedule
RVU Changes 2006 – 2007(includes budget neutrality adjuster)
Medicare Physician Fee Schedule 2007 • Imaging Procedures • Continuation of 2006 policy that reduces technical component by 25% for second and subsequent imaging procedures in the same family • In addition, payment for technical component in freestanding imaging centers (including physician practices) is capped at the hospital outpatient payment rate • When both imaging cuts apply, multiple imaging adjustments are taken first
Imaging Payment Determination for Services Subject to Multiple Imaging Reduction and Hospital OP Cap
Medicare Physician Fee Schedule 2007 • IVIG Preadministration Services • CMS has extended this payment for 2007 • Use code G0332, defined as preadministration-related services for intravenous infusion of immunoglobulin, per infusion encounter; paid at approximately $71 • Bill this code in addition to appropriate drug administration code and J-code for the IVIG • Colorectal Cancer Screening Services • Effective 1/1/07 Medicare has waived the beneficiary deductible requirement for covered CRC screening services; copayments will still apply
Medicare Physician Fee Schedule 2007 • No mention of 2007 Oncology Demo Project in the fee schedule • It is ASCO's understanding that the 2006 Oncology Demonstration Project expired on December 31, 2006 and the codes are no longer payable
Tax Relief and Health Care ActMedicare Improvements and Extension Act of 2006 • Passed by Congress 12/9/06; signed by President 12/20/06 • Freezes Medicare conversion factor at 2006 rate ($37.8975) • Bill does not address SGR or change payment rates beyond 2007 • Extends GPCI floor beyond 12/31/06 • Applies only to GPCI for physician work component • Minimum GPCI value for 2007 will be 1.0 • Especially important for rural providers
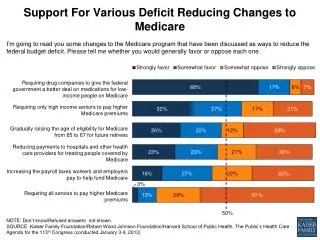
Tax Relief and Health Care Act • Creates 1.5% bonus incentive payment for physicians who report on quality measures • Reporting period will be 7/1/07 – 12/31/07 • Reporting will be based on Medicare Physician Voluntary Report Program (PVRP) measures • CMS has identified 66 measures for 2007; allowed to change the list by posting changes no later than 4/1/07 • Changes to be based on consensus-based process in January 2007
Tax Relief and Health Care Act • 1.5% bonus incentive payment, continued • Measures must be reported for at least 80% of clinically relevant encounters and payment will be calculated based on claims for 2007 services that are submitted by 2/28/08; payment will be made in a lump sum • Further details regarding implementation and oncology-specific measures have not yet been released
Tax Relief and Health Care Act • Establishes a fund ($1.35 billion) to promote physician payment stability and physician quality initiatives in 2008 • Requires that physicians submitting claims for anti-anemia drugs given as part of cancer treatment provide information on hemoglobin or hematocrit levels; effective for drugs furnished on and after January 1, 2008
Tax Relief and Health Care Act • Recovery Audit Contractor program expanded from California, Florida and New York to the entire country • Program allows audit and recovery activity to review claims submitted in fiscal year of the audit and the four prior fiscal years • Requires CMS to have program operating in all states by 1/1/10 • CAP: contractor can now bill Medicare when it ships the drug (subject to returning the money if the drug is never administered), whereas under prior law the contractor couldn't bill until the drug had been administered • CAP drugs now subject to post-payment review
Hospital Outpatient Prospective Payment SystemFinal Rule for 2007 • Payment for drugs, biologics, radiopharmaceuticals • Separately billable drugs paid at ASP + 6% • Medicare will pay separately for drugs costing more than $55 per day; drugs costing less than $55 are not reimbursed separately • Anti-emetics are reimbursed separately regardless of their daily cost • CMS is continuing payment for pre-administration services for IVIG; approximately $75/administration
Hospital Outpatient Prospective Payment System • Drug administration services • New: separate payment for second and subsequent hours of drug administration services • New: CMS will now use all of the CPT codes for drug administration in the hospital outpatient department, instead of the 2006 mixture of CPT codes and C-codes • CMS estimates average 3% increase in Medicare payments for all outpatient services
Drug Reimbursement • Minor changes to the ASP calculation in the fee schedule but no fix to the issue of “underwater” drugs • ASP payment limits continue to be updated quarterly • www.cms.hhs.gov/providers/drugs/default.asp • Still essential to monitor ASP pricing limits and compare to your acquisition costs • ASP was not addressed in the Tax Relief bill
Drug Reimbursement • Drugs administered in the physician office (and hospital OP department) are paid at ASP + 6% with a few exceptions • Drugs furnished through a covered item of durable medical equipment are paid at 95% of AWP as published on 10/1/03. This payment limit will not be updated for 2007. • Payment allowance limits for influenza, Pneumococcal and Hepatitis B vaccines are 95% of AWP • New drugs not included in ASP or NOC pricing files are paid at 106% of WAC or invoice pricing
Competitive Acquisition Program (CAP) • CAP continues as an alternative to ASP + 6% • Very few oncologists have participated • New in 2007: CAP contractor can bill Medicare when it ships the drug rather than waiting until the drug is administered (must return the money if the drug is never administered) • Updated list of drugs available under CAP for 2007 • www.cms.hhs.gov/CompetitiveAcquisforBios/15_Approved_Vendor.asp#TopOfPage
Medicare Part D • 2007 formularies must include all antineoplastic drugs available on 4/1/06 • New antineoplastic drugs must be reviewed for formulary inclusion within 90 days (instead of 180 days as for most drug classes) • The exceptions process is available during the 90 day review period • Specialty tier with non-appealable copay is allowed, but copay is limited to 25%
Coding in 2007 These lists are not all inclusive; check the coding books for additional new codes and/or changes.
ICD-9 Code ChangesEffective 10/1/06 • Increased specificity for hematologic disorders • Myelodysplastic syndrome 238.7x • Neutropenia 288.0x • Drug induced neutropenia 288.03 • Aplastic anemia 284.0 • Elevated white count 288.6x • Decreased white count 288.5x • Neutropenic splenomegaly 289.53 • Myelofibrosis 289.83 • Anemia of chronic disease 285.29
ICD-9 Code Changes • Neoplasm-related pain 338.3 • Mucositis due to antineoplastic therapy 528.01 • Elevated CEA 795.81 • Elevated CA 125 795.82 • Other abnormal tumor markers 795.89 • Elevated PSA 790.93 • Estrogen receptor positive status V86.0 • Estrogen receptor negative status V86.1
CPT Code ChangesEffective 1/1/07 • New patient vs. established patient • A new patient is one who has not received any professional services from the physician or another physician of the same specialty who belongs to the same group practice (same tax ID number), within the past three years • Consultations • Must be requested by a physician or “other appropriate source” • Follow up visits to a consultation are reported using established patient codes in the office/outpatient setting; subsequent hospital care codes in the inpatient setting
CPT Code Changes • Anticoagulation management 99363, 99364 • Not separately payable by Medicare (bundled) • Medical genetics counseling by a genetics counselor 96040 • Not separately payable by Medicare (bundled) • For genetic counseling and education provided by a physician, use Evaluation and Management codes • Additional hours of hydration (90761), therapeutic/diagnostic administration (90766) and chemotherapy administration (96415) no longer have 8 hour time limit
HCPCS Code Changes • Codes of interest • J1562 Immune globulin 100 mg. • J0894 Decitabine 1 mg. • J8650 Nabilone (oral) 1 mg. • J9261 Nelarbine 50 mg. • J1740 Ibandronate sodium 1 mg. • Vectibix continues to be billed with J9999
Drug Administration Services ∙ Hydration ∙ Therapeutic, prophylactic, and diagnostic injections and infusions ∙ Chemotherapy administration
“Initial” service codes • Only one initial code is reported per encounter • The initial code that best describes the key or primary reason for the encounter should be reported, irrespective of the order in which the infusions/injections occur • Subsequent or concurrent codes should be reported for additional infusion/injection services
Each additional hour • Used to report additional hours of infusion, after the first hour, of an individual drug • To report these codes, infusion time must be > 30 minutes beyond the first hour • Infusions lasting 30 minutes or less (after the first hour) should be rounded down and not reported • New in 2007: 8 hour time limit has been removed
Additional sequential infusion • Used for a sequential infusion of an additional substance/drug • Additional hours of sequential infusion are billed using the “each additional hour” codes
Concurrent infusion • The concurrent infusion code (90768) is used when drugs are administered at the same time • Only one concurrent code may be billed per patient encounter • There is no concurrent chemotherapy code • AMA CPT Assistant, November 2006 • “In order to report a concurrent administration, the drugs cannot simply be mixed in one bag; there must be more than one bag.”
Infusion Time • The infusion time begins when the infusion starts. Infusion time reflects the time the drug/substance is actually being administered. Drug preparation time is not included as infusion time. • Rounding • After the first hour of infusion, round infusion times to the nearest 30 minutes. For infusions of 30 minutes or less, round down. For infusions greater than 30 minutes, round up.
Push • Intravenous or intra-arterial push is defined as: a) an injection in which the healthcare professional who administers the substance/drug is continuously present to administer the injection and observe the patient, or b) an infusion of 15 minutes or less.
Therapeutic/diagnostic subcutaneous or intramuscular injections • Use code 90772 for therapeutic/diagnostic sc or im injections • 90772 may be billed for each injection administered during a patient encounter • Use the -59 modifier when reporting injections on the same day as drug administration services • The National Correct Coding Initiative (NCCI) created edits on code 90772 which requires the use of a modifier. If the drug or substance is unrelated to an anesthetic, providers should use the -59 modifier to bypass the edit.
Reminders • Hydration services may be billed only • When it is the only service performed during a patient encounter; or • When it is performed before or after chemotherapy administration (do not bill for hydration at the same time as chemotherapy). Use modifier -59 to indicate a “distinct procedural service”
More Reminders • Evaluation and management services (level 2 through 5) may be reported in conjunction with drug administration services • If a significant separately identifiable E/M service is performed • Bill the appropriate E/M service code with modifier -25 • A different diagnosis is not required
More Reminders • When billing for chemotherapy administration, the following services are included and are not reported separately: • Use of local anesthesia • IV start • Access to indwelling IV, subcutaneous catheter or port • Flush at conclusion of infusion • Standard tubing, syringes and supplies • Preparation of chemotherapy agent(s)
A Training Tool for New Staff:A Building Block Approach to Codingfor Drug Administration • A systematic approach • Why was the patient here? • What did we give them? • How did we give it? • How long did it take? We thank Lawrence Martinelli, MD, Infectious Disease Society of America and CPT Advisor, for the use of these Building Block slides, originally presented at the 2005 CPT Symposium
Why are they here? • The reason for the visit • Sick patient, needs hydration • Chemotherapy administration, will also see provider • Follow up visit, intractable nausea/vomiting, needs drug therapy • This determines which “initial” code to use
What did we give them? • Hydration? • Anti-emetics or other drugs? • Chemotherapy? • This determines which category of administration code(s) to bill • And don’t forget to bill for the J-codes
How did we give it? • IV infusion? • IV push? • SC or IM injection? • A combination? • This determines which specific administration code(s) to bill and if there are concurrent, subsequent, and/or sequential services.
And finally, how long did it take? • ≤ or > 15 minutes (push vs. infusion) • One “hour” • Additional “hours” • Round to nearest 30 minutes • Remember that infusion times are measured by when the infusate is actually running; pre- and post-infusion times are not included • Documentation of start/stop times for each agent is recommended
Role of the Physician Practice Leader • Stay current on Medicare rules and regulations • Reinforce to your partners the importance of Medicare compliance • Work with your state society to establish productive relationships with your Medicare carrier and commercial payers • Support your Practice Administrator as they implement policies to deal with these changes
Role of the Administrator • Update your coding books, reference materials, fee schedule, charge ticket annually or as changes occur • Ensure that your staff is knowledgeable about reimbursement issues for all payers • Establish and implement policies to immediately respond to changes as they occur • Enroll in Medicare list serves to stay up-to-the-minute on changes • Work with local and state societies (oncology societies, MGMA) on reimbursement and policy issues • Work cooperatively with your physician leader in providing leadership for your staff in this challenging environment
ASCO Resources • Coming soon…Practical Tips for the Oncology Practice, 4th Edition • Detailed information about coding, billing, Medicare coverage guidelines • Includes excerpts from Medicare coverage manuals • Available in early 2007
ASCO Resources • Ask a Coding Question • Call 703-299-1054 or • Email practice@asco.org • Cancer Policy Today • E-newsletter for ASCO members; available by request for administrators • Email practice@asco.org
ASCO Resources • Journal of Oncology Practice • Focus on Quality • Practical Tips • For Your Patients • Legal Corner • Research in Practice • Business of the Business • Original Research • Manuscripts and letters to the editor may be sent to jopsubmissions@asco.org