Download
1 / 48
490 likes | 637 Views
Heart Disease. Presence Regional EMS February 2013 CE. Cardiovascular disease is the number one cause of death in the U.S., and many times the first indication of this disease is an acute coronary event

E N D
Heart Disease Presence Regional EMS February 2013 CE
Cardiovascular disease is the number one cause of death in the U.S., and many times the first indication of this disease is an acute coronary event Cardiac arrest is the most severe manifestation of an acute coronary syndrome, and with rapid intervention the EMT can make the difference between life and death Heart Disease
American Heart Association Facts 7 to 8 million people a year seek treatment for chest pain. Of these, 2 million will actually have a cardiac condition that affects the coronary arteries. About 1.5 million will suffer a heart attack. 500,000 of these heart attack patients will die. 250,000 of these patients will die within the first hour of symptom onset.
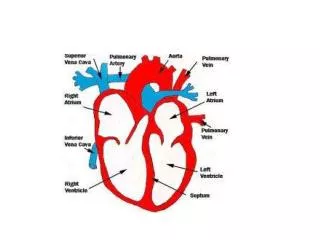
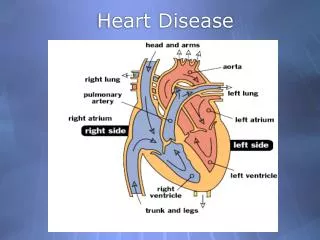
Electric Conduction SA node is primary pacemaker of the heart.
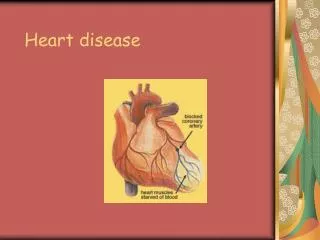
Cardiac Compromise • Cardiac compromise is the result of ischemia, or insufficient blood flow to the heart. • Typically caused by a blockage or narrowing of the coronary arteries. • Will result in tissue infarct, or tissue death, if not corrected.
Normal Artery Artery Clogged with plaque
Pathophysiology of Arterial Blockage • Atherosclerotic changes in the coronary arteries decrease the lumen size and limit the bodies ability to change the vessel sizes (dilation or constriction) when needed. • With plaque rupture, the body sends platelets to the location to try and heal the damage • The platelet aggregation can occlude the artery, hampering blood flow
Acute Coronary Syndrome • Acute Coronary Syndrome, or ACS, is a set of signs and symptoms related to the heart caused by a decrease in blood flow to the heart. • Often due to Atherosclerosis
Acute Coronary Syndrome • Conditions causing cardiac emergencies • Angina pectoris • Stable • Unstable • Myocardial infarction • STEMI (ST Elevated Myocardial Infarction) • NSTEMI (Non-ST Elevated Myocardial Infarction)
Uncontrollable: Age- 83% are >65yo Family history Gender- males are higher risk than females, and have earlier onset of disease Race- African Americans have a greater risk Controllable: Smoking- increases risk 2-4x High blood pressure Diabetes Lack of exercise Stress Obesity Elevated Cholesterol Heart DiseaseRisk Factors
Signs and Symptoms of ACS • Typical or Classic Presentation • Chest pain/pressure/tightness • Pain in arms, neck, jaw, shoulder, back or epigastric area • Shortness of breath or dyspnea • Sweating with out reason • Nausea or vomiting
Signs and Symptoms of ACS • Atypical or Non-Classic Presentation** • Dizzy • Syncope • Anxiety or sense of impending doom • Fatigue ** more likely in females, the elderly and diabetic patients
Complicatons of Acute MI • Sudden Death • Critical Dysrhythmia (advanced providers review dysrhythmias, and their protocols, that can occur) • Cardiogenic Shock • Congestive Heart Failure
Heart Failure • Condition where the heart no longer has the ability to adequately eject blood from the ventricles
Heart Failure • Can also cause Congestive Heart Failure (CHF)
Assessment of ACS Patient • Time is heart muscle • Need to change our mindset for assessment and treatment • National Standard = from the time of arrival at the hospital to cardiac cath lab reperfusion needs to be complete within 90 minutes for best patient outcomes
Assessment of ACS Patient • Scene size-up • Upon arrival, assess the scene for hazards • Determine the need for additional resources • ALS intercept or • Lift assistance • Take appropriate BSI precautions
Assessment of ACS Patient • Initial assessment • Form a general impression of the patient • Unresponsive with no pulse or respirations • Responsive with minor, moderate, or severe distress • Sick or not sick • Determine mental status with AVPU mnemonic • ABC’s • Airway • Open • head tilt chin lift or jaw thrust • Airway adjuncts if needed • Clear (suction if needed)
Assessment of ACS Patient • Initial Assessment (cont) • Breathing (rate and quality) • Adequate • Apply oxygen 15Lpm via NRB mask • Inadequate • Assist ventilation with BVM 10-12 per minute with oxygen 15Lpm • Circulation • Pulse (rate and quality) • If absent begin CPR and AED or Monitor for defibrillation • Assess skins • Determine Priority
Assessment of ACS Patient • History and physical • If the patient is stable: • Gather the SAMPLE and OPQRST history • Perform a focused physical exam • Assess baseline vitals • If the patient is unstable: • Perform a rapid physical exam • Assess baseline vitals • Gather SAMPLE history if available
Assessment of ACS Patient • History and physical • Consider the following SAMPLE questions: • Onset—What were you doing when the pain started? • Provocation or palliation—Do you know of anything that makes the chest pain better or worse? • Quality—Describe the chest discomfort, what is it like? • Radiation—Does the discomfort radiate anywhere? • Severity—How intense is the pain on a 1–10 scale? • Time—When did the discomfort first start, and is it constant or does it come and go?
EMT Basic Provider Care for ACS • Initial Medical Care. • Airway and high flow OXYGEN at 15 lpm per non-rebreather mask. Apply pulse oximeter if available. • Monitor EKG if available. • Transport – consider intercept. • Contact Medical Control. ---------------------------------------- • If patient has own nitro, may assist with administration if approved by Medical Control.
Advanced Provider Care for ACS (1 of 2) • Initial Medical Care. • Airway and OXYGEN at 15 Lpm by non-rebreather. • Monitor. • Consider 12 lead EKG if available. • Per AHA recommendations, complete within 10 minutes of patient contact • Transmit to ED if able • If dysrhythmia or ectopy presents, proceed to appropriate protocol. • NITROGLYCERIN 0.4 mg SL if SBP > 90. • IV of NS at KVO, or saline lock.
Advanced Provider Care for ACS (2 of 2) • Repeat NITROGLYCERIN 0.4 mg SL q 3-5 minutes as long as chest pain persists, to a total of 3 doses. • Monitor vital signs and pain scale prior to each dose; withhold for SBP < 90. • Observe patient for change in symptoms. • If chest pain remains after third NITROGLYCERIN, MORPHINE SULFATE 2 mg IV over 1 minute. • ASPIRIN 325 mg, 1 p.o. • Contact Medical Control. -------------------------------------------------- • Consider additionalMORPHINE SULFATE 2-4 mg IV q 5 minutes.
Medication Review • Nitroglycerin • Action • Vasodilation to increase bloodflow to the heart, decrease workload of heart, and decrease cardiac oxygen demand • Indication • Cardiac related chest pain • Contraindication • Systolic BP<90 • Three doses have already been taken • Pt has taken medication for erectile dysfunction within 24 hours • Route • Sublingual tablet or spray • Dose • 0.4mg tablet or one metered spray every 3-5 minutes until pain resolves up to 3 total doses
Medication Review • Aspirin • Action • Prevents platelet aggregation, or keeps platelets from clumping together • Indications • Cardiac related chest pain • Contraindications • Known allergy • Already had dose today • Route • oral • Dose • 325mg tablet or chewable baby aspirin equivalent.
Medication Review • Morphine • Action • Analgesic and sedative that causes some vasodilation, reducing venous return and reducing myocardial oxygen demand • Indication • Moderate to severe chest pain, and to reduce venous return in pulmonary edema • Contraindication • Allergy, hypotension, volume depletion, acute asthma, COPD, respiratory depression, or pulmonary edema d/t chemical inhalation • Route • IV, IM or Subcutaneous • Dose • For CP protocol, 2mg IV slow over 1 minute, call for additional dosage
Review • Answer the following questions as a group. • If doing this CE individually, please e-mail your answers to: • shelley.peelman@presencehealth.org • Use “Feb 2013 CE” in subject box. • You will receive an e-mail confirmation. Print this confirmation for your records, and document the CE in your PREMSS CE record book.
Scenario You have been dispatched to City Hall for a man ill. En route dispatch tells you it is a 67 yo male in the mayor’s office. As you enter the office you see an older man sitting in a chair. He is pale, sweaty, and has labored respirations. You introduce yourself and he responds with “I feel like” (takes a breath) “I’m gonna die.” You note his respirations to be slightly rapid, but shallow. His radial pulse is normal rate, but irregular.
Scenario • 1. What is your general impression of this patient? Sick or not sick? Why? • 2. What are the rest of the findings of your initial assessment? • 3. What treatment would you initiate at this point?
Scenario • As your assessment continues, the patient tells you he has “stabbing” pain in the middle of his chest that radiates to his left arm. It started 15 minutes ago while he was working at his desk. He rates his pain at an 8/10. His vitals are B/P 180/100, pulse 90 bpm and irregular, rr 26 and shallow. He tells you he had open heart surgery two years ago and takes nitroglycerin, lopressor, and plavix. All of his medications are in his desk.
Scenario • List THREE signs and symptoms of ACS this patient is exhibiting? Are they typical or atypical? • What are you next steps for treatment for your level of training? Advanced providers identify the importance of the prehospital 12 lead EKG.
Questions • Name 5 risk factors for ACS. • List 3 complications of ACS. • What is the action, indication, contraindication, route, and dose of nitroglycerin?
Extra ALS Slides • Identify the following rhythms and outline appropriate treatment. 1. Pt feels “weary and tired”
5. Pt has crushing chest pain radiating into jaw and left arm.