Download
1 / 34
360 likes | 759 Views
Haematological Malignancies in General Practice. Judith Hanslip Consultant Haematologist Lister Hospital, Stevenage. Jon Lambert Consultant Haematologist UCLH & Mt Vernon Cancer Centre. Case 1. 21 year old woman with 3 week history of dry cough and cervical lymphadenopathy

E N D
Haematological Malignanciesin General Practice Judith Hanslip Consultant Haematologist Lister Hospital, Stevenage Jon Lambert Consultant Haematologist UCLH & Mt Vernon Cancer Centre
Case 1 • 21 year old woman with 3 week history of dry cough and cervical lymphadenopathy • Saw GP 3 times over 4 weeks, 2 course of antibiotics • Attended A&E 5 weeks after initial presentation to GP: noted to have signs of SVC obstruction • Urgent CT neck & chest:
Case 1 …necrotic anterior mediastinal mass measuring at least 7x5cm, extending from the thoracic inlet to the right atrium. This is causing severe SVC compression, with a minimum diameter of 1 mm although a patent channel of contrast is seen along its length…
Case 1 • Biopsy – diffuse large B-cell lymphoma • Treated R-CHOP x 6 • Now in CR
Case 2 • 75 year old man, b/g of prostate cancer (quiescent) • 2-week history of backache, followed by unsteadiness on legs, then tingling in fingers • Seen by GP, referred immediately to oncology OP • MRI spine:
Case 2 • Referred immediately to NHNN • Laminectomy C2-T2 and biopsy – plasmacytoma • Bone marrow – multiple myeloma • IgG paraprotein 36g/L, normal renal function & calcium • Started treatment with dexamethasone & velcade
Outline of talk • Epidemiology • Lymphoma • Myeloma • Referral of patients with suspected haematological malignancies
UK Cancer Registrations 2007 HMRN data http://www.hmrn.org/Statistics/Incidence.aspx
Many different subtypes of lymphoma… HMRN data 2012
mostly curable mostly incurable …with very different clinical behaviour Aggressive Indolent Diffuse large B-cell Follicular Hodgkin Mantle cell T-cell Burkitt
Lymphoma – when to suspect • Can affect any organ, and symptoms vary accordingly • Typically present with an enlarging cervical, axillary or inguinal lump • B symptoms are rare and indicate high disease burden • Main question should be: is there an obvious reactive cause for LN?
An isolated node, or the tip of the iceberg? Patient presenting with inguinal lymphadenopathy…
Lymphoma – are any tests helpful? • In most cases of lymphoma, the FBC, biochem and LDH are normal • Only whole-body imaging +/- biopsy are likely to be diagnostic (FNA is no use) • The best guide is from the history and examination
Referral to hospital – when and how quickly? • Rapidly enlarging nodes with systemic or neurological symptoms need urgent referral - discuss same day • Otherwise follow 2-week wait procedure
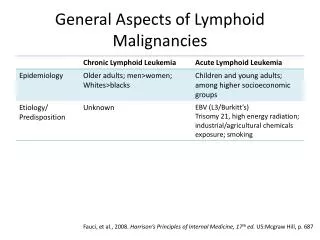
Myeloma – epidemiology • Annual UK Incidence: 40 per x 106 (2500 new cases per year) • Median age at diagnosis 60-65 yrs • Higher incidence in Afro-Caribbean people
Myeloma – epidemiology • 2% under 40 yrs • 35% under 65 yrs
Myeloma – improvements in outcome over 30 years Kumar S K et al. Blood 2008;111:2516-2520
82% 51% 81% 78% 79% n = 11,000 L Ellis-Brookes et al, Brit J Cancer, Sept 2012 Myeloma – route to secondary care… …and its effect on outcome 1-year overall survival
Backache particularly if persistent, unexplained or associated with loss of height and osteoporosis (esp in males and pre-menopausal females) Low blood countsesp normochromic or macrocytic anaemia, but also neutropenia or thrombocytopenia Unexplained renal impairment When to suspect myeloma? • Recurrent infectiondue to ↓immunoglobulins or neutropenia • Hypercalcaemia • Persistent ↑ESR(or plasma viscosity) esp if no obvious infective or autoimmune cause • Spinal cord/nerve root compression
ESR or plasma viscosity FBC U & E, Calcium Protein electrophoresis Immunoglobulin profile Urine for BJP X-rays of painful sites + Skeletal Survey, BM, BJP quantitation Investigations in Suspected Myeloma
Myeloma = M-protein + one of… Bone marrow plasma cells >10% Lytic lesions on skeletal survey Anaemia Hypercalcaemia Impaired renal function Otherwise it’s monoclonal gammopathy of unknown significance (MGUS) M-protein doesn’t necessarily indicate myeloma
Kyle et al, NEJM, March 2006 MGUS Uncommon below age of 50 Risk of progression to myeloma 1% per year
Guidelines for referring patients with suspected haematological malignancies
2010 Patient Experience Survey • 51% of myeloma patients had visited their GP at least 3 times before referralhighest probability of delay out of 24 cancers captured in survey • The overall probability of people with suspected cancer visiting their GPs > 3 times was increased in: • Younger pats • Women • Ethnic minorites