Download
1 / 26
260 likes | 399 Views
Laparoscopy for Splenic Conditions. George W. Holcomb, III, M.D., MBA Surgeon-in-Chief Children’s Mercy Hospital Kansas City, Missouri. Splenic Conditions. ITP Spherocytosis Splenic cysts Wandering spleen. J Pediatr Surg 28:689-692, 1993. Pre-Operative Preparation. Ultrasound

E N D
Laparoscopy for Splenic Conditions George W. Holcomb, III, M.D., MBA Surgeon-in-Chief Children’s Mercy Hospital Kansas City, Missouri
Splenic Conditions • ITP • Spherocytosis • Splenic cysts • Wandering spleen J Pediatr Surg 28:689-692, 1993
Pre-Operative Preparation • Ultrasound • Often done by pediatrician, hematologist • Rarely needed for splenectomy, except may be useful for extremely large spleen • CT Scan – Useful in planning splenic cystectomy • WinRho • Bone marrow stimulant • Usually used to platelet count • Useful pre-operatively to platelet count in ITP pt. • Immunizations –Pneumococcus (Prevnar, Pneumovax)
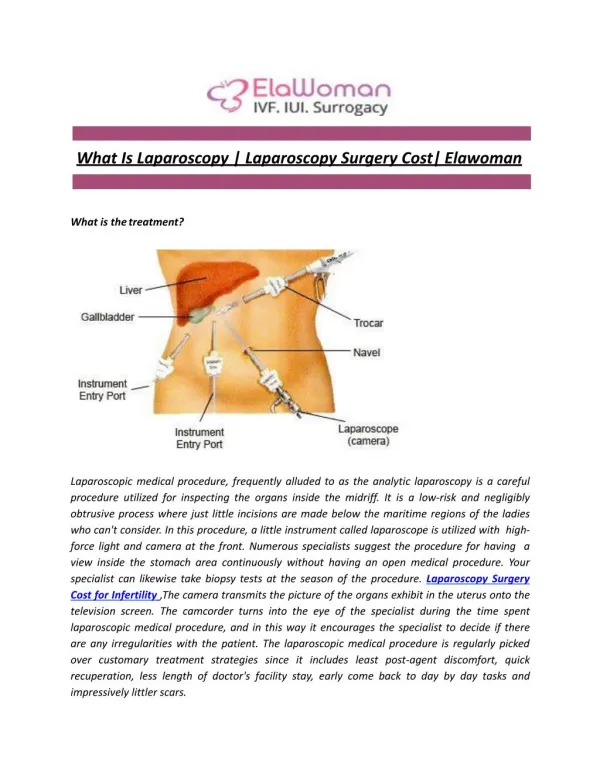
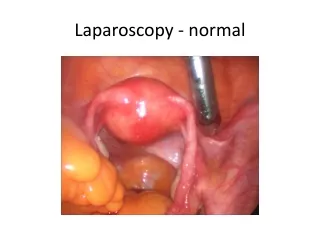
Laparoscopic Splenectomy • ITP, spherocytosis • Port placement • (2) cannulas (5, 12) • (2) stab (3 mm) incisions • Instruments • Harmonic scalpel (5 mm) • Articulating stapler (12 mm)
Laparoscopic Splenectomy Operative Steps • Divide spleno-colic ligament, then short gastrics • Clip artery • Autotransfuse pt • Protects stapler malfxn
Laparoscopic Splenectomy Operative Steps • Divide spleno-renal lig. • Articulating stapler across hilum • Bag specimen, morcellate extracorporally
Laparoscopic Splenectomy Please use this link if you experience problems viewing the video above.
Single Site Umbilical Laparoscopic SurgeryUmbilical Portals (U.S.)
SSULS Splenectomy Please use this link if you experience problems viewing the video above.
Prospective Randomized Trial SSULS vs 4-Port Laparoscopic Splenectomy • Alpha – 0.05 • Power – 0.80 • 60 patients total • 10 patients to date www.cmhclinicaltrials.com
Issues • How large is too large? • 28 cm. – Splenic artery ligation helpful • Can divide spleen (spherocytosis) with harmonic, if necessary
Issues • Postoperative platelet ct. > 500,000 • Reports of splenic vein/portal vein thrombosis following splenectomy (open and laparoscopic) • Baby aspirin ( 81 mg) QD for 6 mos • Re-check at 3 months & 6 months
Splenic Cysts • Primary • epithelial lining • Pseudocysts (secondary) • no epithelial lining • often develop after trauma
Laparoscopic Splenic Cystectomy • First step is decompression of cyst
Laparoscopic Splenic Cystectomy • Excise cyst as close as possible to splenic parenchyma with harmonic scalpel • Coagulate lining with Argon beam coagulator • ? Place omentum adjacent to exposed cyst lining
European Experience • 3 European centers (Mainz, Mannheim, Hannover) • 1995 - 2005 • 14 pts (median 8.5 yr) • 10 recurrences (71%) APSA 2006
Laparoscopic Splenopexy J PediatrSurg 42:E23-27, 2007 Please use this link if you experience problems viewing the video above.
I.U. Experience1995 - 2006 231 patients • Mean age 7.7 yrs • Lap splenectomy – 223 • 211 - total • 12 - partial • Lap splenic cystectomy – 6 • Lap splenopexy - 2 Ann Surg, in Press
Ileus - 5 Bleeding - 4 Acute chest syndrome- 5 Pneumonia - 2 Portal vein thrombosis - 1 HUS - 1 Diaphragm perforation 2 Colon injury - 1 Port site hernia - 1 Total splenectomy after partial - 1 Recurrent cyst - 1 I.U. Experience1995 – 2006Complications 11% overall, 22% in SCD Ann Surg, in Press
QUESTIONS www.cmhmis.com