Download
1 / 74
740 likes | 977 Views
Innovative Treatment Options for Pelvic Organ Prolapse. Travis L. Bullock, MD. Epidemiology of POP. A condition in which the pelvic organs (bladder, uterus, or rectum) “fall” onto the vaginal wall and in some patients bulge outside the vagina.

E N D
Innovative Treatment Options for Pelvic Organ Prolapse Travis L. Bullock, MD
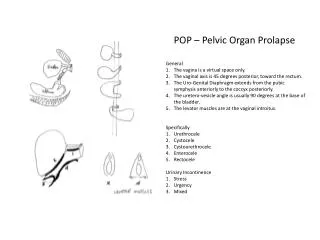
Epidemiology of POP • A condition in which the pelvic organs (bladder, uterus, or rectum) “fall” onto the vaginal wall and in some patients bulge outside the vagina. • A type of “hernia” due to weakening of the muscles and connective tissues of the pelvis. • Affects 50% of women, however only 20% of those women have significant symptoms. • Unfortunately, only about half of these women seek medical help despite a significant impact on their quality of life.
Epidemiology of POP • One of the most common gynecologic surgeries performed • >500,000 procedures performed annually • > $1 Billion spent yearly on surgery alone • 11% lifetime risk of surgery by 80yo • Up to 30% will have >1 surgery for POP highlighting the high failure rate of current procedures
Projected Female Population • Population of women >60yo is expected to increase by 72% • Women >60yo are more likely to seek care than their younger counterparts
Prevalence of Pelvic Floor Disorders • Demand for services to care for pelvic floor disorders will increase at twice the rate of the growth of the general population!
Risk Factors • Age • Parity • Family history of prolapse (collagen) • Post menopausal state • Repetitive pressure on the pelvis (constipation, chronic cough, obesity) • Prior pelvic surgery such as hysterectomy. • Caucasian 3X more common than African American women
Prolapse Symptoms • Many women may have no symptoms. More advanced prolapse may experience some or all of the following: • Vaginal or rectal pressure • You may feel or see a bulge protruding from the vagina • Difficulty emptying the bladder • Inconsistent urinary stream • Trapping of stool in the rectum • The need to place a finger in the vagina to empty the bladder or bowel • Vaginal irritation • Low backache • Spotting of blood on the underwear • Recurrent bladder infections
Types of Prolapse • Named for the anatomic area or organ prolapsing • Anterior wall = Cystocele • Posterior wall = Rectocele • Apical Prolapse • Enterocele • Uterine prolapse • Vaginal vault prolapse • Often have more than one type of prolapse
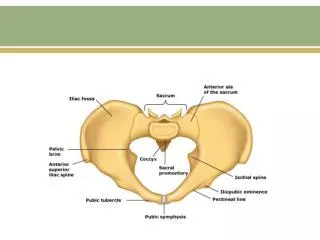
Anatomy of Pelvic Support • Boney pelvic framework • Endopelvic fascia • Levator ani muscles • Collagenous connective tissue attachments to the pelvic side walls
Anatomy of Pelvic Support • Level I: Parametrium and paracolpium (Uterosacral and Cardinal ligaments). Supports the upper 1/3 of vagina • Level II: Direct lateral attachments to the arcus tendineus (pubocervical fascia). Supports the mid 1/3 of vagina • Level III: Vagina fuses with urethra and perineal body. Supports distal 1/3 of vagina.
Evaluation • Examine in lithotomy position • Standing if degree of prolapse does not correlate with symptomatology • Bottom blade of speculum • Valsalva or cough vigorously and note relationship of pelvic organs • Rectovaginal exam • Perineal body • Vaginal mucosa (atrophy, fissures, ulcers) • Incontinence with and without prolapse reduction • PVR
Baden-Walker or “Half-way” system • Easy to use and widely understood • Most dependent position of pelvic organs during maximal straining • 1st degree • Half-way to the hymen • 2nd degree • To the hymen • 3rd degree • Beyond the hymen
Prolapse Grading • 4 grades popularized by Raz • 1: minimal hypermobility of the bladder • 2: bladder base to introitus with straining • 3: bladder base outside introitus with straining • 4: bladder base outside introitus at rest
POP-Q • In 1996 ISC/AUGS developed the POPQ • Standardized, site specific system to quantify and classify POP • Measurements at 9 specific sites relative to the hymen • Inter-examiner and Intra-examiner reproducibility • Can be bulky and time consuming • Used mostly for research
Treatment Options for POP • Non-surgical • PFME and Behavioral techniques • Pessary • Surgical • >100 procedures described • Colporrhaphy • Sacrospinous fixation • Mesh augmentation • Sacral Culpopexy • Open • Laparoscopic • Robotic
Non-surgical Treatment • Behavioral changes • Weight loss, avoiding heavy lifting, correcting a chronic cough (quitting smoking), or preventing constipation that contributes to straining to have a bowel movement. • Pelvic floor exercises (Kegels) • Cannot reverse the prolapse, but contracting strong pelvic floor muscles when lifting or bearing down may prevent pelvic organ prolapse from becoming worse or help relieve symptoms. • Vaginal pessary • the most common non-surgical treatment for prolapse.
Vaginal Pessary • Worn in the vagina to support prolapsed organ • Must be specially fitted • Removed for periodic cleanings • May be associated with vaginal discharge and erosions • Favorable risk-benefit ratio
Colporrhaphy • Plication of fibromuscular tissues of vaginal wall • Most common prolapse procedure performed • Minimally invasive • May be associated with vaginal scaring or shortening • 10-70% failure rate, 30% reoperation rate
Sacrospinous Ligament Fixation • Attachment of the apex of the vagina to the sacrospinous ligament • Often combined with colporrhaphy • Hysterectomy not always required • Technically challenging • Extensive dissection and retraction may be required • Deviates the vagina
Mesh Augmentation • Substitute “damaged” tissues with synthetic material • Decreased recurrence rate as compared to traditional plication • Easy to perform with familiar trocar passes • Can be associated with pain and erosions if not familiar with the technique • Short term data is favorable, but still maturing
Mesh Augmentation • American Medical Systems • Apogee, Perigee, Elevate • Gynecare • Prolift • Bard • Avaulta • Boston Scientific • Pinnacle, Uphold
Sacral Culpopexy • “Gold Standard” for uterine and vaginal vault prolapse • A graft if used to suspend the vagina to the inside of the sacrum • Maintains anatomical position • Preserves vaginal axis and maintains vaginal length • Low recurrence rate • Traditionally performed with an abdominal incision • Can be completed laparoscopically using the da Vinci robotic system
Open (abdominal) Good long-term results: 93-100% success rates with durable repair Increased morbidity: invasive mid-line incision leading to prolonged recovery time (5-6 hospital days) 5% of all prolapse procedures Laparoscopic Reproduce open approach minimally invasively Technically difficult learning curve due to complex suturing and dissection Now Robotic … Sacral Culpopexy
History of Robotics in Medicine • Term “robot” was first coined in 1921 by the Czeck writer Karel Capek is his play Rossum’s Universal Robots • Robota = forced labor
History of Robotics in Medicine • 1985-PUMA 560 CT guided brain biopsy • 1987-first CCK with robotic assistance • 1998-PROBOT for transurethral resection • 1992-ROBODOC (Integrated Surgical Supplies) used in orthopedics
History of Robots in Medicine • 1993-AESOP (Computer Motion, INC). First robot approved by the FDA • 1998-Zeus • Surgeon control center and 3 robotic arms. • First fully endoscopic robotic procedure (CABG) • Computer Motion and Intuitive Surgical merged in June 2003 • 2000-da Vinci Surgical System.
da Vinci Surgical System • Approved by the FDA in 2000 for laparoscopic surgery • Surgeon console and patient side robotic cart with 3 or 4 arms • “Master-Slave” surgical system • High-Definition 3-D Visualization • EndoWrist instruments • >800 in use in the United States and Europe • Cost = $1.2-1.75 million