Download
1 / 34
370 likes | 852 Views
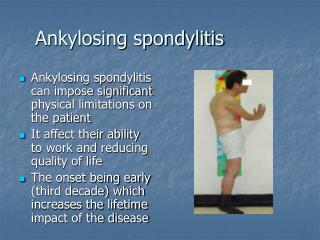
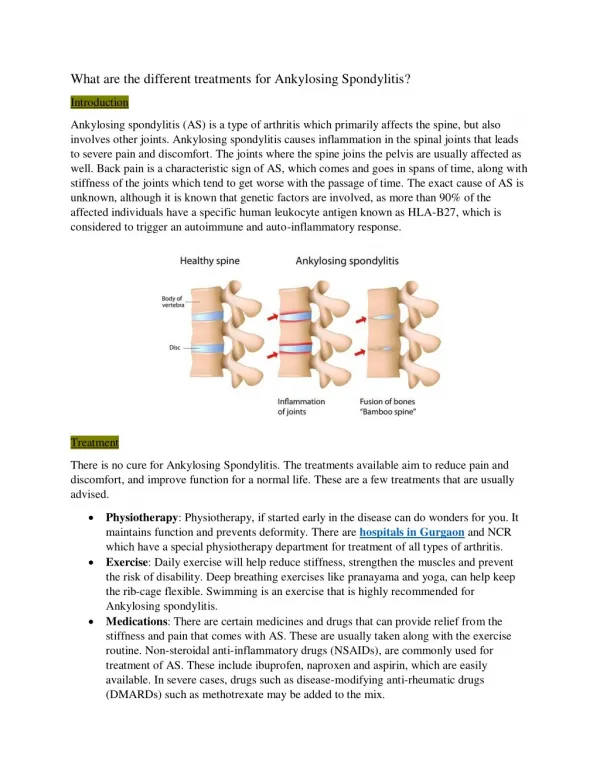
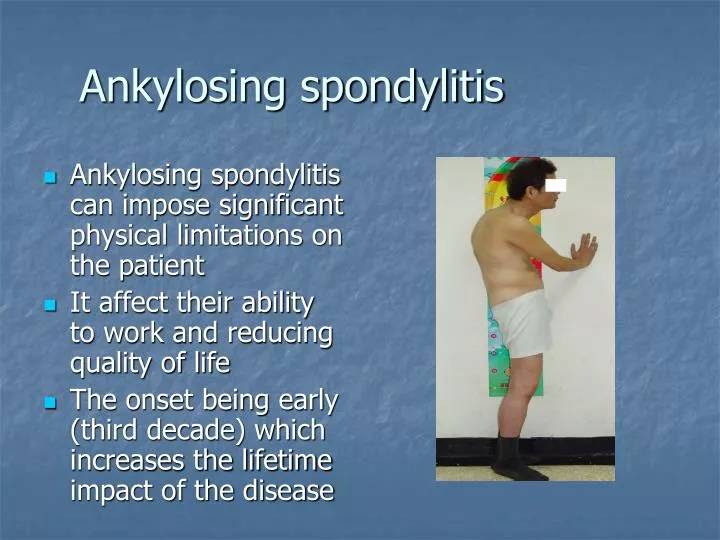
Ankylosing spondylitis. Ankylosing spondylitis can impose significant physical limitations on the patient It affect their ability to work and reducing quality of life The onset being early (third decade) which increases the lifetime impact of the disease. Ankylosing spondylitis.

E N D
Ankylosing spondylitis • Ankylosing spondylitis can impose significant physical limitations on the patient • It affect their ability to work and reducing quality of life • The onset being early (third decade) which increases the lifetime impact of the disease
Ankylosing spondylitis • Delay in diagnosis • Recent survey of 1614 patients with AS illustrate the protracted delay between onset and Diagnosis • Average of 8.9 years mean delay of making Dx. • In women the mean delay 9.8 vs 8.4 in Males(probably due to misconception thatonly men are affected)
Ankylosing spondylitis • Relative sensitivity of detecting active Sacroilliitis : MRI Plain Radiography Quantitative Scintigraphy MRI 95% Plain radiography 19% QS 48% J Rheumatol 1996;23-2107-15
Ankylosing spondylitis • Only 50-70% of AS patients with active disease exhibit biological markers of inflammation with elevated ESR and CRP • Relative late appearance of radiographic sacroiliitis , by up to several years after first symptoms
Ankylosing spondylitis • Symptoms early in the disease are due to inflammation • Symptoms later in the disease are caused by a mixture of inflammation , structural spinal damage and secondary damage to soft tissue such as muscles and ligaments.
Ankylosing Spondylitis • Predictive factors for long term outcome: -Hip arthritis is the strongest predictive factor being associated with 23-fold increase in the risk of severe arthritis Other factors: • Age-onset before 16 • High ESR • Unresponsive to NSAID • Limitation of lumbar spinal movement
Ankylosing spondylitis • About 60-75% of patients with AS show good to very good response to full dose NSAIDs in 48 hours , in contrast with only 15% of patients with mechanical back pain. • Recent study has shown that patients with AS treated continuously over two years with a daily dose of NSAIds has less radiological progression compare to those who took NSAIDs on demand Arth Rheum 2005;52-1756-65
Ankylosing spondylitis • 20-50% of AS patients still have active disease despite treatment with NSAID. • For those patients , Anti-TNF have meant a breakthrough in treatment
Ankylosing spondylitis -MRI follow up studies during treatment with etanrcept and infliximab have shown that acute inflammatory lesions in the spine and sacroiliac joints can be effectively suppressed , bony destruction and proliferation can be prevented
Etanercept in AS Sustained durability and tolerability for 96 weeks.A&R 2005-64:1557-62 -277 AS patients who were enrolled in RCT (257 continued open labeled Etanrcept. AS patients continuing Etanrcept Rx had sustained response for almost 2 years • Improvement is symptoms , signs and spinal mobility • None of the most serious safety concerns :TB, drug induced lupus, MS or lymphoma were reported .
Outcome in Active AS, Clinical and MRI data , 2-years A&R December 2005 • 26 patients with active AS treated with etanercept 25mg twice weekly • Conclusion : The clinical efficacy and safety of etanercept in patients with active AS without simultanous administration of DMARDs or steroids over 2 years of continuous treatment is confirmed • Spinal inflammation as depicted by MRI decreased significantly.
Ankylosing Spondylitis ASAS/EULAR recommendations for Management of AS 22 expert participants: Ten Key recommendations for the treatment of AS were developed and assessed using a combination of research based evidence and expert consensus.
Ankylosing Spondylitis • 1- Treatment of AS should be tailored according to: - Current Manifestations of the disease -Level of current symptoms, clinical findings and prognostic indicators -General clinical status -Wishes and expectation of the patient
Ankylosing Spondylitis • 2-Disease Monitoring: -patient history -clinical parameters -laboratory tests -Imaging All according to clinical presentations and ASAS core set Frequency of monitoring should be decided on symptoms, severity, and drug treatment
Ankylosing Spondylitis • 3-Optimum therapy of AS requires pharmacological and non-pharmacological treatment
Ankylosing Spondylitis • 4-Non-pharmacological treatment of AS : -Patient education -regular exercises -physical therapy -Patients associations and self help groups may be useful.
Ankylosing spondylitis • 5- NSAIDs are recommended as first line therapy for treatment of AS with pain and stiffness. • In those with increased GI risk , selective COX2 inhibitors could be used.
Ankylosing spondylitis • 6- Analgesics may be used for pain in whom NSAID are insufficient, contraindicated and or poorly controlled.
Ankylosing spondylitis • 7- Corticosteroids injections directed to the local site of inflammation may be considered. • The use of systemic steroids for axial disease is not supported by evidence.
Ankylosing spondylitis • 8-There is no evidence for the efficacy of DMARDs including SSZ and MTTX for the axial manifestations . • SSZ may be considered in patients with AS and peripheral arthritis.
Ankylosing spondylitis • 9-Anti-TNF Rx should be given to patients with persistently high disease activity despite conventional treatment • There is no evidence to support the obligatory use of DMARDs before or concomitant with anti-TNF treatment in patients with axial disease
Ankylosing spondylitis • 10-Total hip arthroplasty should be considered in patients with refractory pain and disability and radiographic evidence of structural damage. • Spinal surgery-for example corrective osteotomy and stabilization procedure may be value in selected cases.
Ankylosing spondylitis • First International ASAS consensus statements for the use of Anti-TNF agents in patients with ankylosing spondylitis • Published online ARD August 2005 • Guidelines for the use on Anti-TNF in AS
Ankylosing spondylitis • -Anti-TNF therapy is considered as a major advances (breakthrough) in the treatment of AS patients • There is a need to identify i-patients with active disease ii-Patients with threatening functional disability iii-patients who may have most benefits from Rx.
Ankylosing spondylitis • Etanrcept 25mg biweekly and infliximab 5mg/kg every 6-8weeks are approved in US and Europe for the treatment of signs and symptoms of patients with active AS • Adalimumab is not yet approved for AS ( US and EUROPE)
Ankylosing spondylitis • Only patients with active disease should be considered for treatment with antiTNF agents Active disease as indicated by both • 1- BASDAI score of =or>4 and • 2- physician global assessment of =or>2 on a Likert Scale (1=mild,2=moderate, 3=severe , 4=very severe) should be present to warrant anti-TNF therapy
Ankylosing spondylitis • Failure to respond to at least 2 NSAIDs , each NSAID should have been used for at least 3 months at maximum dose • Failure treatment of at least one DMARD for peripheral arthritis (SSZ or MTX)
Ankylosing spondylitis • Assessment of response to Rx is recommended after 6-8 weeks. • Improvement Criteria : Improvement in BASDAI of=or > 2 in BASDIA score and physician global assessment of =or>1
Ankylosing spondylitis • Discontinuation of Anti-TNF : • If the response criteria are not met within 6-8 weeks , it is recommended to D/c the anti-TNF agents • The use of other anti-TNF may be considered.
Ankylosing spondylitis • There is no available data that active MRI and high CRP are required to support therapy with anti-TNF in individual patient
Ankylosing spondylitis • Conclusion: • AS can and has to be diagnosed earlier than is being done at present even before radiological changes are evident • Therapies with NSAIDs and TNF blockers are most effective for the signs ,symptoms that are caused by inflammation.
Ankylosing Spondylitis • The disappearance of inflammation in the spine and sacroiliac joints during treatment, as detected by MRI is a demonstration of great efficacy of TNF blockers and also suggests that structural damage may also be prevented • Ann Rheum Dis 2005-0nline
Ankylosing Spondylitis • Whether and how these new treatments also have the potential to induce long term remission if given early enough has to be shown in the future. • Ann Rheum Dis 2005-0nline