Download
1 / 65
660 likes | 923 Views
ALTITUDE MEDICINE. Shawn Dowling Sept 2008. Discuss basic altitude physiology How to recognize altitude disorders Management Prevention. Will not discuss: Subacute/Chronic Altitude Illnesses Cold-related illnesses Altitude-exacerbated illnesses. Objectives. High Altitude Illnesses.

E N D
ALTITUDE MEDICINE Shawn Dowling Sept 2008
Discuss basic altitude physiology How to recognize altitude disorders Management Prevention Will not discuss: Subacute/Chronic Altitude Illnesses Cold-related illnesses Altitude-exacerbated illnesses Objectives
High Altitude Illnesses • Definition • Cerebral (AMS HACE spectrum) and pulmonary (HAPE) syndromes which develop in un- or underacclimatized persons after ascent to high altitude • Are often PREVENTABLE and can usually be managed if S/Sx are recognized early and Tx are implemented in a timely fashion
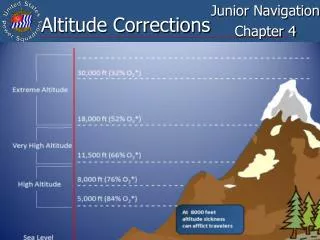
Moderate Altitude • 2400-3000m (8,000-10,000ft)- i.e. Lake Louise/Sunshine Valley • Minor impairment of arterial oxygen transport (SaO2>90%), PAO2>60 torr • Usually not clinically important unless significant underlying medical disorder • AMS common with rapid ascent above 2500 meters
High Altitude • 3000-5500m (10,000-18,000ft) • i.e. Mount Columbia (12, 365ft – highest point in Alberta) • Maximum arterial saturation < 90%; PAO2<60 torr • Most common range for serious altitude illness
Extreme Altitude • 5500-8850m (18,000-29,035ft) from Mount Logan (19550ft) to Mount Everest (29035ft) • Marked hypoxemia and hypocapnia • Maximum arterial saturation 50-75%; PAO2 28-40 torr • Deterioration eventually outstrips acclimatization, complete acclimatization not possible
More About Gas! At sea level we are underneath an ocean of air % O2 is always 21% But as you climb higher, the Patm drops and thus your PO2 drops PiO2 = 0.21(PB-47) PB=barometric pressure At sea level PiO2= 160 mm Hg At 2500m PiO2 = 119 mm Hg Aconquilcha,Chile 5340m PiO2 = 82 mm Hg On top of Everest (8848m) PiO2 = 43 mm Hg Thanks Rigby
Acclimatization • Complex adaptation by essentially every system to minimize hypoxia and maintain cellular functions despite decreased PiO2 • Given sufficient time most people can acclimatize to 5500m/18150ft, beyond that progressive deterioration occurs
So WHAT IS the problem with Altitude? • HYPOXIA • WHAT ARE THE PHYSIOLOGIC COMPENSATIONS? • Essentially all the physiologic changes are attempting to improve arterial and therefore cellular oxygenation
Pulmonary Response to PiO2 • Hypoxemic Ventilatory Response • Begins w/i minutes of ascent above 1500m • Hypoxia - pulmonary vasoconstrictor • Allows for selective shunting away from areas of hypoxia w/preferential areas of vasodilation • pulmonary vascular resistance • pulmonary artery pressure (cold and exercise PAP while descent, O2 and certain Rx PAP) • diffusion capacity and lung volume
Hypoxemic Ventilatory Response • Ventilation increases proportionally to the degree of hypoxia detected at the chemoreceptors • Lower PaCO2 = higher PAO2 • remember … PAO2 = PiO2 - PaCO2/R • As PCO2 drops a respiratory alkalosis occurs (what does this do to the medulla?) • kidneys compensate by excreting bicarb(over 6-8/7) • Vigourous HVR helps acclimatization whereas a poor HVR may lead to altitude-illness
HVR Carotid bodies O2 Aortic bodies
Cerebral Circulation • Hypoxemia = increases cerebral blood flow • Hypocapnea = decreases cerebral blood flow • Net result is an increase (modest) in cerebral blood flow at PaO2 <60 (altitude >12,500 feet) • Contributes to pathophysiology of AMS and HACE
CVS Response • Catecholamine release: Epi and Norepi • Sympathetic Tone: • CO= HR x SV • BP= CO x PVR • This responses allows for better tissue perfusion (but, also decreases exercise performance) – over time epi/norepi levels drop and CO/HR/PVR return to normal
Hematologic • Blood volume increases immediately: • Primarily due to hemo[ ] from diuresis • Hypoxia stimulates renal EPO production • Takes weeks for it to effect Red Cell Mass • Oxygen Dissociation curve – combination of inc 2,3 DPG (rightward shift) and alkalosis (leftward shift) leads to minimal net effect
Gotta know it. It’ll be on the exam!
High Altitude Illness • What are RF? • What are positive predictors? • What worsens altitude illnesses? • What does not effect altitude illnesses?
High Altitude Illness • What are Risk Factors? • Rate of ascent/Starting altitude • Altitude reached • Sleeping at altitude • Individual physiology/Genetics? • What are Positive Predictors? • Hx of prior ascent w/o Sx • Elderly (less AMS/HACE), Women (less HAPE)
What worsens altitude-illnesses? • Respiratory depressants/Alcohol • Pre-existing Medical Illnesses (very few): i.e. Pulm HTN, certain CHD, • Exertion • Hypothermia • What does not affect risk? • Physical fitness • CAD/HTN • Mild COPD • Pregnancy • DM
Case #1 • You’ve decided to hike to Machu Picchu and have flown directly from Lima (sea level) into Cuzco (3515m/11,600ft). That day you start the hike up and notice you develop a nasty HA, and nausea.
What’s your Diagnosis? • Acute Mountain Syndrome • High Altitude Cerebral Edema • High Altitude Pulmonary Edema • Other Medical Illness
Pearl • Any illness at altitude is altitude illness until proven otherwise.
Lake Louise Criteria for AMS • Presence of a HA in an un-acclimatized person who has arrived at an altitude >2000m (usu >2500m) • + 1 of • GI (anorexia, N,V) • Fatigue • Insomnia • Dizziness/lightheaded • Sx usually begin between 6-10 hrs but may be as early as 1 hour
Pearls • Never ascend with symptoms of AMS • Never leave someone with AMS alone -Letting someone with AMS hike alone is the equilavent of going for a hike in the Kananaski’s alone the night of Party at the retreat.
Treatment? • Any or Combination • Stop, Rest and Continue once Sx resolve • Acetazolimide (alone or in combination) • Dexamethasone • O2, immediate descent • Nifedipine • + Symptomatic Treatment
Treatment? • Any or Combination • Stop, Rest and Continue once Sx resolve • Acetazolamide (alone or in combination) • Dexamethasone (if severe) • O2, rapid/immediate descent • Nifedipine • + Symptomatic Treatment
Treatment Options of AMS • Stop and rest at altitude that Sx 1st develop +/- Acetazolamide -> May proceed once Sx abate • + Tx Sx • Nausea: Prochlorperazine 10mg po/im (stimulates HVR) • HA: Tylenol/NSAID’s • Insomnia: acetazolamide 125mg PO QHS
Treatment of AMS Mild Symptoms Does not need descent if mild Sx and constant supervision Stop ascent until better Acetazolamide (250 BID) Tylenol/ASA for Sx Anti-emetic PRN Consider O2 at 1-2 LPM Moderate or Unresolving AMS Descent 500 m Consider: O2 at 1-2 LPM Hyperbaric therapy Dexamethasone 4mg PO q6h until able to descend May ascend after symptoms resolve
If someone is getting worse, go down at once • If Sx of HACE are present DESCEND IMMEDIATELY
Quick word about Acetazolamide • What’s the MOA?
Quick word about Acetazolamide • What’s the MOA? • Causes a bicarb diuresis by inhibiting Carbonic Anhydrase at the kidney • This leads to a metabolic acidosis which counteracts the alkalosis from hyperventilation • Allowing an individual to have a better HVR and therefore acclimatize better • Which allergy must you ask about?
Pt adamant that the HA is from dehydration • Can give Dx/Tx of 1L of fluid + advil or tylenol – if this completely resolves HA, not likely to be AMS
Case #2 • Despite the advice to refrain from continuing to ascend, you continue up and begin to feel disoriented and noticed you seem to be walking with a drunken’ sort of gait • Dx?
High Altitude Cerebral Edema (HACE) • Least common but most lethal altitude illness • Usually occurs above 3600m(12,000 feet) • Symptoms usually develop over 1-3 days • reported range 12 hours to 9 days • Usually also have symptoms of AMS / HAPE
HACE Dx • Presence of a change in mental status and/or ataxia in a person with AMS Or • Presence of both mental status changes and ataxia in a person without AMS
HACE S & Sx • Think of the effect of hypoxia and ICP • Global encephalopathy • Ataxia • Altered mentation • Seizures • Occasional CN palsies (secondary to increased ICP) • Papilledema • Retinal hemorrhage • Coma • Death is due to brain herniation
Tx of HACE • DESCENT (until pt improves) • O2 • DXM 8mg PO/IM/IV initially then 4mg Q6H • +/- acetazolamide 250mg PO BID • What if the weather does not allow for a safe descent and you happen to be part of a well equipped expedition?
Gamow Bag • Hyperbaric Chambers • Lightweight (14.9 lb) • Manually pressurized • Generate 103mm Hg (2 psi) above ambient pressure • Simulates descent of 4000-5000 feet at moderate altitudes • Simulates descent of 9000 feet at top of Mt. Everest • After short course of treatment patient often able to descend on their own • This is primarily a temporizing measure - Not an alternate to descending
Case #3 • During a visit to Nepal, Mr. Hackalung, decides to organize a hike to Everest Base camp (5430m/18000ft). • On day 3 you notice you notice he develops a dry cough and during the lunch break he’s quite SOB • You’re the group doc • What’s the most likely Dx?
Fortunately for you, you realize that you develop X-ray vision at altitude – convenient skill – except that you’re on an all guy expedition but…- here is what you see. Case #3
High Altitude Pulmonary Edema (HAPE) • Responsible for most high altitude deaths • Relatively Abrupt Onset • Usually occurs on 2nd night at altitude, Rare after 4 days • Women less susceptible than men • Presence of HAPE increases likelihood of cerebral illnesses – by worsening hypoxemia: 50% have AMS & 14% have HACE