Download
1 / 12
231 likes | 1.22k Views
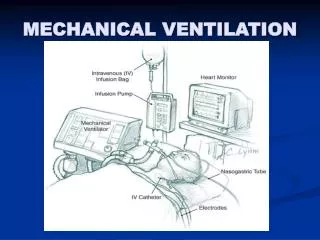
ACLS: Airway Management: Endotracheal Intubation. Dr. Linda Frasca Edward Via Virginia College of Osteopathic Medicine Block 12. Indications: Endotracheal Intubation. Respiratory Failure: Hypoxia, Hypercapnia, tachypnea, or apnea ; ie. ARDS, asthma,

E N D
ACLS:Airway Management:Endotracheal Intubation Dr. Linda Frasca Edward Via Virginia College of Osteopathic Medicine Block 12
Indications: Endotracheal Intubation • Respiratory Failure: Hypoxia, Hypercapnia, tachypnea, or apnea ; ie. ARDS, asthma, pulmonary edema, infection, COPD exacerbation • Inability to ventilate unconscious patient • Maintenance or protection of an intact airway • Cardiac Arrest • Medication administration
Contraindications: • Inability of patient to extend head • Moderate to severe trauma to the cervical spine or anterior neck • Infection in the epiglottal area • Mandibular fracture or trismus • Mild hypoxia • Uncontrolled oropharyngeal hemorrhage • Intact tracheostomy
Equipment • Laryngoscope • Blades: curved (MacIntosh) and straight (Miller) • Endotracheal tubes of various sizes: • Neonates and full term infants: no. 0 and 1 • Adult women: 7.0 mm i.d. tube • Adult men: 8.0 to 8.5 mm i.d. tube • Pediatric size: (age in years/4) + 4 or width of fingernail of the fifth digit
Continue Equipment for ET intubation: • Lubricant, Malleable stylet • 10-ml syringe (to inflate ET cuff) • Oxygen and manual bag valve mask • Suction apparatus • Stethoscope • Sterile gloves and goggles • Oropharyngeal airway • CO2 Detector
How do you confirm the correct placement of the ET Tube? • Primary Confirmation • Secondary Confirmation
Primary Confirmation By Physical Exam • Confirm tube placement immediately • Listen over the epigastrium and observe the chest wall for movement • If stomach gurgling and no chest wall expansion, esophagus intubated:remove ET tube • Reattempt intubation after reoxygenation
Primary Confirmation: cont. • If chest wall rises and stomach not gurgling, perform 5-point auscultation • If still doubt, use laryngoscope to see the tube passing through the vocal cords (best) • Secure the tube • Look for moisture condensation on the inside of the tracheal tube (not 100%: false + with esophageal intubations)
Secondary Confirmation • End-Tidal CO2 Detectors • Commercial device that reacts with a color change to CO2 exhaled from the lungs: MELLO YELLOW • Qualitative detection device indicates exhaled CO2 indicates proper tracheal tube placement • Absence of CO2 (unless prolonged CPR), indicates esophageal intubation • False+: Distended stomach, carbonated beverages • False-: Low or no blood flow state ( as above)
Endotracheal tube(ET) trachea, endotracheal tube (arrows) and location of carina (^). University of Virginia
Complications • Hypoxia • Long duration of procedure • Esophageal intubation ( not visualizing vocal cords) • Intubation of a bronchus ( right more common) • Failure to secure the placement • Failure to recognize misplacement of tube • Aspiration • Pneumothorax
Complications: continued • Trauma and adverse effects • Broken teeth • Oral lacerations • Vocal cord injury • Pharyngeal-esophageal perforation • Short-term laryngeal edema • Release of high levels of epinephrine and norepinephrine stimulated by tracheal intubation: can cause elevated blood pressure, tachycardia, arrhythmias