Download
1 / 23
280 likes | 612 Views
Invasive Aspergillosis. Guha , et al. Infect Med 24 ( Suppl 8): 8-11, 2007. 34-year-old woman Presents with 2-day history of weakness, dizziness, left calf pain, and black tarry stools. Denies chest pain, cough, or shortness of breath Medical history:

E N D
Invasive Aspergillosis Guha, et al. Infect Med 24 (Suppl 8): 8-11, 2007 • 34-year-old woman • Presents with 2-day history of weakness, dizziness, left calf pain, and black tarry stools. • Denies chest pain, cough, or shortness of breath • Medical history: • Diabetes leading to renal failure and renal transplant • 3 weeks before presentation, acute graft rejection developed • Began an immunosuppressive regimen
Invasive Aspergillosis Guha, et al. Infect Med 24 (Suppl 8): 8-11, 2007 • On admission • Tachycardic, hypotensive and febrile • Initial chest x-ray was normal • Lab results: • Anemia • WBC = 4800/µl, 80% neutrophils • Blood cultures were positive for E. coli • Antibiotic therapy initiated
Invasive Aspergillosis Guha, et al. Infect Med 24 (Suppl 8): 8-11, 2007 • Day 6: • Vesicular rash developed on buttocks and left calf • Cultures positive for HSV, antiviral therapy initiated • Day 8: • Renal function continued to decline • Intermittent hemodialysis started • Day 12: • Decreased responsiveness • Intubated for respiratory distress
Invasive Aspergillosis Guha, et al. Infect Med 24 (Suppl 8): 8-11, 2007 • Chest x-ray: • Diffuse bilateral lung nodules • Culture of BAL: • Positive for Aspergillus spp. • Immunesuppression decreased • Liposomal Amphotericin B started • Condition deteriorates: • Acute MI, comatose • Mulitple acute infarcts in frontal lobe and cerebellum by MRI • Multiple skin nodules form on arms and trunk
Invasive Aspergillosis Guha, et al. Infect Med 24 (Suppl 8): 8-11, 2007 • Culture of skin nodule biopsy: • Aspergillus spp.
Aspergillosis • Epidemiology: • Most common fungus worldwide – Ubiquitous • Hospital acquired infection - Major problem • Virulence factors and pathogenesis: • Thermo-tolerant to 50C • Elastase, phospholipase, protease and catalase • Conidia bind to fibrinogen and laminin • Invasive disease is dependent on impaired neutrophil function • Unable to generate the oxidative burst to kill AT RISK: Severe neutropenia, leukemia and lymphoma.
Aspergillosis - Clinical Aspects Clinical Manifestations: • Route of infection: Inhalation • Incubation: days to weeks • Forms of infections: • Allergic aspergillosis • Cavitary colonization - aspergilloma • Primary pulmonary aspergillosis • Invasive aspergillosis
ABPA – Allergic broncopulmonary aspergillosis (ABPA) • Asthma • Pulmonary infiltrates • Peripheral eosinophelia • Elevated serum IgE • Hypersensitivity to Aspergillus antigen • Skin test
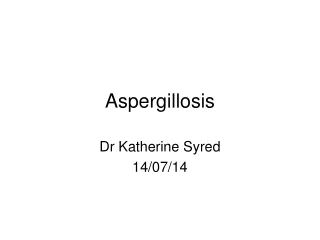
Aspergilloma • Colonization of paranasal sinuses and the lower airways • Obstructive bronchial aspergillosis • Occurs in pre-formed cavitary lesions • Cystic fibrosis • Chonic bronchitis • TB • No tissue damage, asymptomatic
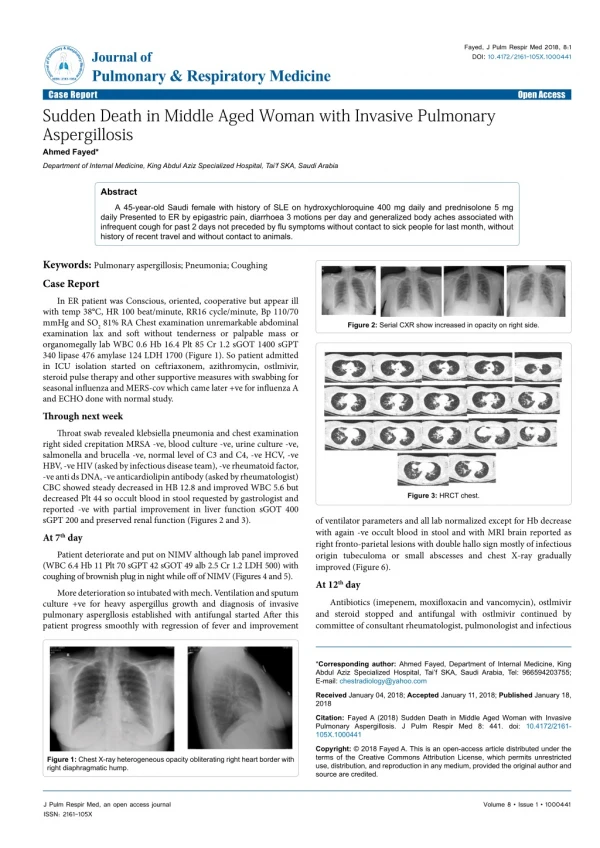
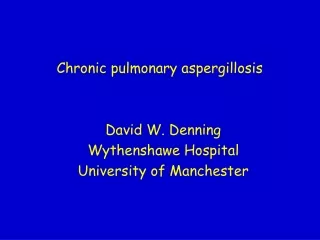
Aspergillosis – Laboratory Diagnosis • Laboratory Diagnosis: • Monomorphic true mould • Difficult because of the universality of the fungus • REPEAT ISOLATIONS ARE ESSENTIAL FOR DEFINITIVE DX • Serum: galactomannan Ag + invasive aspergillosis • Histopathology: • Septatehyphae • dichotomous branching at ACUTE angles • May see full conidial structures (i.e. fruiting bodies) • In culture: • A. fumigatus – “rapid grower” • Septate, hyaline hyphae • conidiophores with phialides • pointing upwards, bearing chains of conidia
Aspergillosis Direct prep from tissue specimen Acute, dichotomous branching
Aspergillosis Septate hyphae Aspergilloma Conidiophore “fruiting body”
Aspergillosis A. fumigatus
Aspergillosis - Treatment • Treatment: • Invasive disease is difficult to treat • Amphotericin B, caspofungin (echinocandins), voriconazole • Decrease immunosuppression or reconstitute immune defenses • Surgical debridement, if possible • Prevention in high-risk patients: • Neutropenic: Filtered air to minimize exposure!
Invasive Aspergillosis Guha, et al. Infect Med 24 (Suppl 8): 8-11, 2007 • Our patient: • Expired on hospital day 23 • At autopsy, A. flavuswas detected in multiple organs: • Heart, lungs, adrenal galnd, thyroid, kidney, and liver • Extreme example of disseminated aspergillosis in an immunocompromised host
Opportunistic hyalohyphomycoses • Diverse agents • Many are ubiquitous – inhaled conidia • Many are resistant to antifungal agents • In tissue, they appear indistinguishable from Aspergillus! (i.e. branching, septate hyphae) • Repeated isolation from multiple sites/multiple times is best criteria to determine clinical significance. BOTTOM LINE: CULTURE IS CRITICAL FOR DX & TREATMENT
Opportunistic hyalohyphomycoses FusSceAcrPae • Disseminated infection is increasing in incidence • Some examples: • Fusarium(R to ampB), immune reconst. + new triazoles • Scedosporium(R to ampB) – surgical resection • Acremonium (S unestablished) • Paecilomyces– voriconazole • …and many, many more.
Phaeohyphomycoses • Many are neurotropic: • present as brain abscesses, sinusitis CNS BOTTOM LINE: • Response to therapy is unpredictable between genera • Culture is critical for diagnosis and therapy
Phaeohyphomycoses Alt Cur BipCla • In tissue: • Pigmented hyphae w/ or w/o yeast are present • Disseminated infection is increasing: Alternaria, Curvularia, Bipolaris, Cladosporium…and others
Pneumocystosis • Etiology: Pneumocystisjirovecii • Most common opportunistic infection among individuals with AIDS • Incidence has decreased significantly with HAART • Reservoir in nature unknown • Pneumonia is clearly the most common presentation • Interstitial pneumonitis, mononuclear infiltrate • Onset insidious • Diagnosis based on microscopic examination of BAL