Download
1 / 22
230 likes | 291 Views
Learn about Benign Prostatic Hyperplasia (BPH) and Prostatic Carcinoma, with clinical features, complications, histology, PSA staining, and prostate cancer spread. Understand Testis Tumors, Seminoma, Teratoma, and more in Testicular Cancers.

E N D
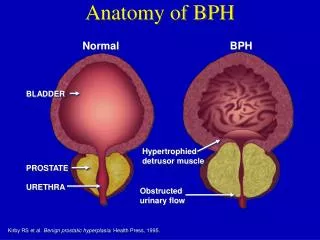
PROSTATE GLAND: • Benign nodular prostatic hyperplasia (BPH) • non-neoplastic enlargement • common > 50y • recurrent urinary infection • eventually renal function • Morphology • both lateral lobes + ‘median lobe’ • cut surface: • multiple solid nodules /some cystic areas • histology: hyperplasia of glands and stroma • Clinical features • Obstructive symptoms • 2 factors: • hyperplastic nodules • distortion of course of prostatic urethra • peri- urethral zone involvement interferes with • sphincter mechanism • Obstructive symptoms
Complications • Continuedobstruction: • hypertrophy of bladder musculature • trabeculation / diverticulae if compensatory mech. fails • dilatation of bladder hydroureter hydronephrosis Also: • incomplete bladder emptying • residual urine infection (bladder) • also ascending pyelonephritis / septicaemia - renal function / ± stones
Prostatic carcinoma • one of commonest cancers • 2nd most NB cause of ♂ † from malignancy • usually > 50 y (peak 60-85) • adenocarcinoma in posterior sub-capsular area • invasion of stroma / perineural spaces • osteosclerotic bone metastases (pelvis + other sites) • gross findings on cut surface: • tumour ill-defined, gray or yellow, firm • histology: • adenocarcinoma usually moderately / well differentiated • Gleason grading system 1 (well) 5 (poor diff.) • correlates with clinical behaviour PSA stain useful to confirm origin from prostate in cases of metastases
in some cases especially elderly patients a microscopic focus of • tumour is found incidentally • ‘dormant lesions’ • rather low risk of metastasis • Mode of spread of prostate carcinoma • •direct • - stromal invasion • - prostatic capsule • - urethra, bladder base, seminal vesicle • • via lymphatics to nodes • - sacral • - iliac • - para-aortic • • via blood to bone (osteosclerotic) • - pelvis • - lumbo-sacral spine • - femur • - lungs • - liver
Testis • Tumours: • - relatively uncommon • important – young men • highly malignant improved prognosis with • chemo • Aetiology • maldescended testis • 10 x higher risk • Classification: • Germ cell NB (85 – 90 %) • Non-Germ cell • Germ cell • Seminomas • Teratomas
Classification in use: • Seminoma (most common) • Teratoma ( less common) • Combined / mixed (seen, but less common) • Malignant lymphoma • Yolk sac uncommon • Leydig cell tumour • + others
Seminoma • commonest type • germ cell origin • peak incidence 30 – 50 years • Morphology: • testes enlarged by homogenous firm white • solid tumour (potato-like) • Histological subtypes • Classical seminoma: - commonest • histology: • uniform cells, clear / vacuolated cytoplasm • lymphocytic infiltrate, granulomatous reaction • other histological types less common • may also have precurser lesions ajacent to • tumour – called intra-tubular germ cell neoplasia • seminomaspreads to para-aortic nodes • good prognosis • very radiosensitive
Teratoma • Germ cell origin • Peak incidence 20-30 y • More aggressive than seminomas • composed of several types of tissue (variably • differentiated) representing: • endoderm - bowel type mucosa, etc. • ectoderm - skin, appendages,neural • mesoderm – cartilage, fat, mesenchymal
Classification of Teratomas • difficult • - prognostic relevance • differentiated • undifferentiated (malignant)somatic and/or extra • embryonic differentiation (yolk-sac/choriocarcinoma) • 2 Classifications: UK and USA (WHO) • UK:USA (WHO) • Differentiated same • Malignant • Malignant undifferentiated embryonal carcinoma • (WHO) • Malignant trophoblastic choriocarcinoma • (WHO)
- differentiated - rare - malignant teratoma (variably differentiated) - partly solid / cystic - poorer differentiated extensive tumour necrosis with haemorrhagevariegated appearance on cut surface • some may contain trophoblastic tissue • choriocarcinoma (haemorrhagic) • associated serum(HCC) human chrorionic • gonadotrophin, ( AFP) also yolk-sac/ embryonal • carcinoma components • aggressive tumours with vascular invasion • blood-borne metastases common
Combined germ cell tumours • seminoma / teratoma intermingled • teratoma component determines prognosis • Yolk-sac tumour • - pure type • usually before 3 years • in adults – usually one component of mixedgerm • cell tumour • AFP raised in serum
Non-germ cell tumours • Primary malignant lymphoma • uncommon • elderly • bi-lateral • non-Hodgkin B-cell lymphoma (testes may be) • secondarily involved in cases of widespread • seeding of an underlying • primary lymphoma i.e. • lymphoblastic lymphoma in children
Tumours of the penis • 2 types • • Intra-epidermal carcinoma (Bowen’s disease) • rare • sharply circumscribed erythematous (red) patch • risk for invasive squamous carcinoma • • Invasive squamous carcinoma • more common Africa / Asia • only in uncircumcised males • papilloma virus may play role • glans / inner part of foreskin • nodule / plaque ulcer • histology: well differentiated squamous carcinoma • invades corpora • metastases:inguinal lymphnodes • Carcinoma of scrotum • rare • previously described in chimney sweeps – occupational • exposure to carcinogens
Bladder • Pathological changes following chronic cystitis • von Brunn cell nests develope as a result of nests of • urothelial cells becoming trapped in inflammatory • fibrous tissue in chronic cystitis • may become cystic • cystitis cystica • show glandular metaplasia • cystitis glandularis Tumours • most bladder tumours are transitional cell(TCC) • carcinomas • squamous cell / adenocarcinomas are far less common • sarcomas rare • aetiological factors for TCC include: - exposure to • dyes (aniline compounds) • chronic smoking • analgesic abuse • aetiological factors for squamous cell carcinoma • include • schistosomiasis (bilharzia) • calculi
Transitional cell carcinoma • - arises from urothelium • frequently multiple • ‘field effect’ • often preceded by dysplasia • Morphology • most are papillarywith delicate fronds • covered by variably atypical urothelium • Histology: • Low and High-grade tumours • Low-grade: • papillary • cells show minimal atypia • usually no invasion • good prognosis High-grade: • less papillary • solid, usually invasive • severe cellular atypia • high grade may show squamous / glandular • metaplasia • poor prognosis
Carcinoma in situ • often multi-focal change between tumours • precursor for invasive tumour • Squamous cell carcinoma • arises from metaplastic epihelium • schistosomiasis / calculi • usually solid / invasive • poorer prognosis than TCC • Adenocarcinoma • uncommon • arises from: • urachal remnants • cystitis glandularis • peri – urethral / prostatic glands • TCC with glandular differentiation • Mesenchymal tumours • uncommon • benign: - leiomyoma etc. • malignant:rhabdomyosarcoma • Children (embryonal) – polypoid ‘grape-like’ called • sarcoma botryoides
Adults – rhabdomyosarcoma (straited muscle) • Secondary tumours: • direct extension • • cervix • • prostate • • rectum
Obstructive uropathy • Causes: • Infancy:congenital anomalies: • uretero – pelvic stenosis • vesico – ureteric reflux • urethral valves • Puberty to middle-age (females) • - short urethra predisoses to • ascending infection with • - minor trauma • - pregnancy • 40 + years (men) – prostatic disease (BPH) • - less common calculi • - cancer bladder / • advanced prostate cancer • all ages – instrumentation (catherisation, • cystoscopy) • - underlying diabetes
Pathogenesis • pelvic and calyceal system become dilated due to • back pressure (mild in acute obstruction) • gross dilation result of prolonged back pressure • hydroureter / nephrosis • kidney becomes dilated sac-like structure • loss of functional kidney tissue
Urinary calculi (stones) • 1-5% of population (UK) • mainly 30+ • > males • common in renal pelvis • Causes • substance in excess (precipitation to form • stone) • factors affecting solubility abnormal (citrates, • others inhibit ) • factors also NB: • pH • mucoproteins from nidus • Classification • According to composition • Ca-oxalate (± Ca-phosphate / uric acid) commonest • triple stones – Mg/Am/ PO4 • may form large ‘staghorn’ stones - uric acid stones
NB: 90% of patients with Ca-containing stones have idiopathic hypercalcuria with normal serum Ca 10% - hyperparathyrodism or other cause of hypercalcaemia
Mg/Am /PO4 (triple) stones: • associated with UTI (Proteus) organisms • - change urea ammonia • alkaline conditions + flow precipitation • staghorn may form • chronic irritataion metaplasia carcinoma if very longstanding Uric acid stones: • gout • radiolucent