Download
1 / 1
10 likes | 204 Views
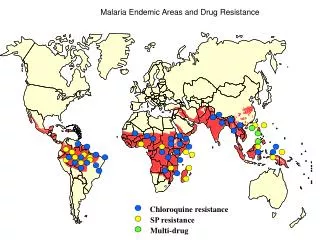
Introduction Malaria can be seasonal, with precipitation playing a key role. East Africa has significant wet and dry seasons. Mosquito populations increase during wet seasons. Chloroquine was the drug of choice, but resistance developed. Resistance decreased as other drugs were used.

E N D
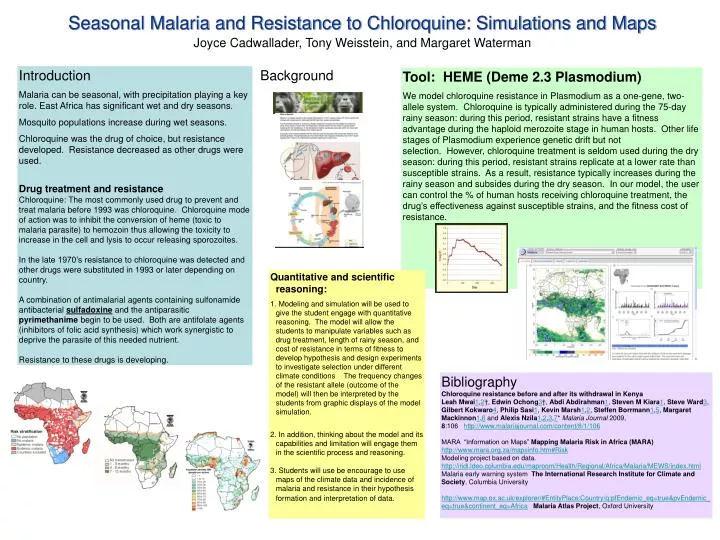
Introduction Malaria can be seasonal, with precipitation playing a key role. East Africa has significant wet and dry seasons. Mosquito populations increase during wet seasons. Chloroquine was the drug of choice, but resistance developed. Resistance decreased as other drugs were used. Drug treatment and resistance Chloroquine: The most commonly used drug to prevent and treat malaria before 1993 was chloroquine. Chloroquine mode of action was to inhibit the conversion of heme (toxic to malaria parasite) to hemozoin thus allowing the toxicity to increase in the cell and lysis to occur releasing sporozoites. In the late 1970’s resistance to chloroquine was detected and other drugs were substituted in 1993 or later depending on country. A combination of antimalarial agents containing sulfonamide antibacterial sulfadoxine and the antiparasitic pyrimethanime begin to be used. Both are antifolate agents (inhibitors of folic acid synthesis) which work synergistic to deprive the parasite of this needed nutrient. Resistance to these drugs is developing. Background Tool: HEME (Deme 2.3 Plasmodium) We model chloroquine resistance in Plasmodium as a one-gene, two-allele system. Chloroquine is typically administered during the 75-day rainy season: during this period, resistant strains have a fitness advantage during the haploid merozoite stage in human hosts. Other life stages of Plasmodium experience genetic drift but not selection. However, chloroquine treatment is seldom used during the dry season: during this period, resistant strains replicate at a lower rate than susceptible strains. As a result, resistance typically increases during the rainy season and subsides during the dry season. In our model, the user can control the % of human hosts receiving chloroquine treatment, the drug’s effectiveness against susceptible strains, and the fitness cost of resistance. • Quantitative and scientific reasoning: • 1. Modeling and simulation will be used to give the student engage with quantitative reasoning. The model will allow the students to manipulate variables such as drug treatment, length of rainy season, and cost of resistance in terms of fitness to develop hypothesis and design experiments to investigate selection under different climate conditions The frequency changes of the resistant allele (outcome of the model) will then be interpreted by the students from graphic displays of the model simulation. • 2. In addition, thinking about the model and its capabilities and limitation will engage them in the scientific process and reasoning. • 3. Students will use be encourage to use maps of the climate data and incidence of malaria and resistance in their hypothesis formation and interpretation of data. Seasonal Malaria and Resistance to Chloroquine: Simulations and Maps Joyce Cadwallader, Tony Weisstein, and Margaret Waterman Bibliography Chloroquine resistance before and after its withdrawal in Kenya Leah Mwai1,2†, Edwin Ochong3†, Abdi Abdirahman1, Steven M Kiara1, Steve Ward3, Gilbert Kokwaro4, Philip Sasi1, Kevin Marsh1,2, Steffen Borrmann1,5, Margaret Mackinnon1,6 and Alexis Nzila1,2,3,7* Malaria Journal 2009, 8:106 http://www.malariajournal.com/content/8/1/106 MARA “Information on Maps” Mapping Malaria Risk in Africa (MARA) http://www.mara.org.za/mapsinfo.htm#Risk Modeling project based on data. http://iridl.ldeo.columbia.edu/maproom/Health/Regional/Africa/Malaria/MEWS/index.html Malaria early warning system The International Research Institute for Climate and Society, Columbia University http://www.map.ox.ac.uk/explorer/#EntityPlace:Country/q:pfEndemic_eq=true&pvEndemic_eq=true&continent_eq=AfricaMalaria Atlas Project, Oxford University