Download
1 / 22
220 likes | 360 Views
Renal Cancer: Front line therapy. Walter Stadler. Pathology. Clear cell (conventional) Fuhrman grading 1-4 Papillary Type 1 & 2 (by histology) OR Class 1 & 2 (by molecular profiling) Mucinous -tubular and spindle? Clear-cell papillary Chromophobe

E N D
Renal Cancer: Front line therapy Walter Stadler
Pathology Clear cell (conventional) • Fuhrman grading 1-4 Papillary • Type 1 & 2 (by histology) OR Class 1 & 2 (by molecular profiling) • Mucinous-tubular and spindle? • Clear-cell papillary Chromophobe • Genetically related to benign oncocytoma Collecting duct • Genetically related to urothelial • Medullary (only in sickle cell trait or disease) TFE-3 translocation tumor • Same translocation as alveolar-soft part sarcoma • More than one translocation Renal Cancer|
Clear cell subtypes By VHL status • Wild type (12%) • HIF-1/HIF-2 express (57%) • HIF-2 express (30%) 2 – 4 clusters by expression profile • mRNA • miRNA Brannon, et al, Genes Cancer, 2010 Gordan, et al; Cancer Cell, 2008 Beroukhim, et al; Cancer Res, 2009 CGA Network, Nature, 2013
Other important alterations Histone modification gene mutatations • SETD2 (histone H3 methyltransferase, ~15%) • JARID1C (histone H3 demethylase) • UTX (histone H3 demethylase) Chromatin remodeling complex mutations • PBRM1 (~40%) • BAP1 (~15%) Ubiquitin E3 ligase complex alterations • SPOP overexpression in 99% ccRCC PI3K/AKT/mTOR pathway activation (28%) Dalgliesh, et al; Nature, 2010 Varela, et al; Nature, 2011 Liu, et al, Science, 2009 Kapur, et al. Lancet Oncol, 2013 CGA Network, Nature, 2013
International prognostic model Manola J et al. Clin Cancer Res 2011;17:5443-5450
AG013736 X X Sunitinib Sorafenib Pazopanib Axitinib X
Time(months) Bevacizumab/IFNA Outcome Overall Survival Progression Free Survival 1.0 --Bev/IFNA: median PFS 8.4 months IFNA: Median PFS 4.9 months HR= 0.71 (95% CI=0.6-0.8) Stratified log-rank p<0.0001 ----BEV/IFN:Median OS 18.3 months IFN: Median OS 17.4 months Stratified log-rank p=0.069 1.0 0.8 0.8 0.6 0.6 0.4 0.4 0.2 0.2 0.0 0 6 12 18 24 30 36 42 48 0.0 Time(months) 0 6 12 18 24 30 36 42 48 54 60
Kinase interaction map Sorafenib Sunitinib Karaman, et al Nature Biotech. 26:127, 2008
First line: Sunitinib vs IFNA Total Death Sunitinib 190 IFN-a 200 9
Motzer RJ et al. N Engl J Med 2013;369:722-731. Kaplan–Meier Estimates of Progression-free Survival According to Independent Review. First line: Sunitinib vs Pazopanib
First line: Axitinib vs Sorafenib The Lancet Oncology Volume 14, Issue 13 2013 1287 - 1294
VEGF pathway inhibitor toxicities Hall, et al. J Am CollCardiol HF, 2013 • Cardiac (~73%) • Hypertension • Reversible Posterior Leukoencephalopathy • MI • CVA • CHF • Integument • Hand/Foot • Mucositis • Diarrhea • Systemic • Fatigue • Dysgeusia • Metabolic • Liver toxicity • Hypothyroidism
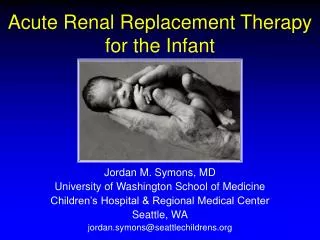
mTOR Inhibitors Sirolimus (Rapamycin) Temsirolimus Everolimus (RAD001)
First line: Temsirolimus vs IFNA Renal Cancer|
Comparative and sequential data R A N D O M I Z E** Everolimus10 mg/day Sunitinib50 mg/day*** Study endpoints SCREEN • Primary • PFS-1st line • Secondary • Combined PFS • ORR-1st line • OS • Safety Cross-over upon progression 1 : 1 Everolimus10 mg/day Sunitinib50 mg/day*** N = 471 1st Line 2nd Line *NCT00903175. **Stratified by MSKCC prognostic factors. ***4 weeks on and 2 weeks off. Motzer, et al; ASCO 2013
Sunitinib versus everolimus sequential Renal Cancer|
mTOR toxicities • Metabolic • Hyperglycemia • Hyperlipidemia • Increased creatinine • Integument • Diarrhea • Mucositis • Pruritic rash • Systemic • Fatigue • Edema • Pneumonitis • Infectious risks • Hematologic • Thrombocytopenia
mTOR inhibitors *Poor prognosis only, included non-clear cell
Non-clear cell: comparative trials Sunitinib vs Temsirolimus • Central European Society for Anticancer Drug Research • Accrual complete, 22 pts total Sunitinib vs Everolimus • Duke sponsored multi-institutional • Accrual complete Sunitinib vs Everolimus • MDAnderson sponsored • 108 planned
RCC front line therapy VEGF pathway directed agents are active in clear cell RCC • Sunitinib, Pazopanib, Sorafenib, Axitinib and Bevacizumab/IFNA improve PFS • There are biochemical and side-effect profile differences, but little clinical differences • Pazopanib is first line reference standard mTOR inhibitors are active in RCC • Temsirolimus improves survival of poor prognosis RCC over IFNA • Role of mTOR inhibitors is decreasing Immunotherapy is active • HD-IL2 leads to long term complete responses, but only in ~5% of highly selected patients • PD1 pathway inhibitors likely to play a role
RCC front line therapy Current pragmatic decisions based on side effect profiles Future decisions must be based on pathologic and molecular sub-typing Renal Cancer|