Download
1 / 52
1.39k likes | 5.7k Views
An approach to Respiratory Distress in Newborn. By Goh Kiam Seong HTAR, Klang 2011. Plan. Introduction Causes and Classification Respiratory Distress Signs Evaluation and Investigation General Management. Introduction. Respiratory Distress in Newborn

E N D
An approach to Respiratory Distress in Newborn By GohKiamSeong HTAR, Klang 2011
Plan • Introduction • Causes and Classification • Respiratory Distress Signs • Evaluation and Investigation • General Management
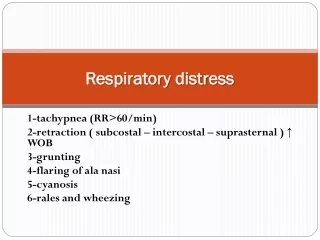
Introduction Respiratory Distress in Newborn = Abnormal respiratory signs in neonates
Tachypnoea Respiratory Rate: < 1 week up to 2 months: 60 or more 2 to 12 months: 50 or more 12 months to 5 years: 40 or more
Tachypnoea • Retractions • Due to negative intrapleural pressure generated between the contraction of diaphragm, respiratory muscles and the mechanical properties of lung and chest wall • Suprasternal Retraction SSR • Intercostal Retraction ICR • Subcostal Retraction SCR
Expiration through partially closed vocal cords to increase airway pressure and lung volume resulting in improved ventilation-perfusion (V/P) ratio • Low pitched expiratory sound. • Protective phenomenon to prevent collapse of alveoli: PEEP • Grunting
Video – Baby Grunting • Grunting Baby pt. 2.flv
Narrow nasal space contributes to total lung resistance • Nasal flaring decreases the work of breathing • Nasal Flaring
Cyanosis • Clinical detection of cyanosis depends on total amount of desaturated HB in blood • Anaemic infants may have low PaO2 that is missed clinically • Polycythaemic infants with normal PaO2 can appear cyanotic
Cyanotic Baby • Pink Baby
What respiratory distress signs you can see here in this child? Central cyanosis, +ICR, +SCR, +NF
Potter face: abnormal facies with a beak nose, receding chin, broad nasal bridge, epicanthal folds, and large low set ears
Meconium stained Nail Meconium stained Cord
Silverman Anderson Score for Premature Baby Score > 6 = impending Respiratory Failure Downe’s Score for Term Baby
Look for: • O2 Saturation • Metabolic/ respiratory acidosis/ alkalosis • Blood counts (Hb/TWC/Plt/Ht) • Glucose level • Sepsis causative agent • Collapse/Air Leak/CDH/ Cardiomegaly
General Management O2 Delivery PEEP/ Mechanical ventilation (CPAP/SiPAP) Intubation and suction • HR monitoring • Continuous SPO2 monitoring • Temp/DXT monitoring • I/O charting • Feeding (PO/TPN) • Cot/Incubator nursing • According to diagnosis
Definition • PRS is a facial difference caused by underdevelopment of the lower jaw • Characterised by: • Micro- and retrognathia • glossoptosis • respiratory obstruction • With or without cleft palate. • Incidence = 1:8500-14000 birth • =
Because underdeveloped lower jaw begins a sequence of events which leads to abnormal position of tongue and cleft palate. PRS is a sequence not syndrome!
Aetiology • Unknown • Recently identify may be caused by genetic anomalies at chromosomes 2, 11, or 17
PRS is often part of an underlying disorder or syndrome • Stickler syndrome • Velocardiofacial syndrome • Fetal Alcohol syndrome • Treacher Collins Syndrome
Pathophysiology At 12 -14/52 GA
How to diagnose? • Only by examining the patient at birth Complication • Difficulties in breathing and feeding.
GERD more prevalent in children with Robin sequence. (Dudkiewicz, CPCJ Mar 2000)
Our tactics • Position: Keep in prone or lateral position • Feeding: Tube feeding or Haberman feeder • Nutrition: Increase daily calorie intake • SPO2 monitoring
Other considerations • Endotracheal intubation/tracheostomy • Tongue lip adhesion • Ophthalmology follow up – if suspect Sticker syndrome (possible retinal detachment) • Mandibular distraction (distraction osteogenesis) • Cleft palate reparation (6.5 mo- 2 yo)
ChoanalAtresia • Choanalatresia is a congenital disorder where choana is blocked by abnormal bony or soft tissue formed during fetal development • Cause: unknown (thin tissue separating the nose and mouth area during fetal development remains after birth) • Most common nasal abnormality in newborn (1 in 7,000 live births) • : = 1 : 2 • >50% associated with other congenital disorder • Diagnosed shortly after birth
Types • Unilateral • Bilateral • Membranous • Osseous
Symptoms and Signs Cyanosis during feeding Pink while crying
Inability to nurse and breathe at same time • Inability to pass a catheter through each side of the nose into the throat • Persistent one-sided nasal blockage or discharge
Associated conditions • Coloboma • Heart defects • Retardation of growth or mental development • Genital/urinary abnormalities • Ear anomalies/deafness IF associated with all these ~ CHARGE syndrome (defect in Chromosome 8 CHD7 gene)
Tests that may be done include: • CT scan • Endoscopy of the nose • Sinus x-ray