Download
1 / 19
220 likes | 552 Views
Delusions and Dementia. Vaughan Bell. Institute of Psychiatry, King’s College London. Outline. Idiopathic psychoses vs psychosis in dementia Neuropsychology Impact and clinical correlates Treatments: drug and non-drug Conclusions. Early Onset Psychosis.

E N D
Delusions and Dementia Vaughan Bell Institute of Psychiatry, King’s College London
Outline • Idiopathic psychoses vs psychosis in dementia • Neuropsychology • Impact and clinical correlates • Treatments: drug and non-drug • Conclusions
Early Onset Psychosis • More males than females, high genetic loading, weakly associated with cognitive impairment. • Most common delusions (Appelbaum et al., 1999) • Persecutory (51.1%) • Body / mind control (26.5%) • Grandiose (23%) • Religious (18%) • Thought broadcasting (6%)
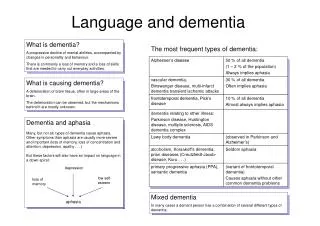
Late / Very Late Onset Psychosis • More females than males, low genetic loading, weakly associated with cognitive impairment. • Most common delusions (Howard et al., 1993) • Persecutory (93.3%) • Passivity (17.2%) • Grandiose (14.9%) • Note also that ‘partition’ delusions and ‘phantom boarder’ delusions are also reported as common (Hassett, 2005)
Delusions in Dementia • No consistent sex difference, virtually no genetic loading, strongly associated with cog. impairment. • Most common delusions (Ballard et al., 1995) • Reference (22%) • Theft or hidden possessions (22%) • Phantom boarder (21%) • Persecution (17.7%) • Misidentification (14.5%) • NB: Other reviews have put persecutory as most prevalent.
Delusions in Dementia • Interestingly, molecular genetic studies have suggested specific risk markers for delusions. • Zdanys et al. (2006) reported ApoE ε4 allele carriers at higher risk specifically for delusions in AD. • This is not a gene identified in mol. genetic studies of idiopathic psychosis. • ApoE ε4also increases risk for AD, younger onset of AD but seemingly not cognitive decline in AD.
Prevalence and Incidence (Prob. AD) • Prevalence: Bassiony and Lyketos (2003) • Clinic sample: 16% - 70% (median 36.5%) • Population: 15% - 22% • Incidence: Devanand et al. (1997) • 6 month transition probability of 17%
Cumulative Incidence (Prob. AD) Cumulative % of delusions by year after diagnosis Paulsen et al. (2000)
Functional Neuroanatomy • Neuroimaging studies on dementia typically implicate right frontal dysfunction. • There seems to be less temporal involvement than in the idiopathic psychoses.
Functional Neuroanatomy • Some suggestion of theme linked to regional changes. Resting PET - Sultzer et al. (2003) Healthy AD No Delusions AD Delusions
Cognitive and Clinical Correlates • Cognitive decline, particularly executive deficits, have been linked with psychosis in AD (Schneider and Dagerman, 2004) • …although is not consistently linked with psychosis in dementia per se (Bassiony and Lyketos, 2003) • However, delusions in AD predict aggression, wandering, functional impairment, worse general health and more severe depression. • Possibly as 1/3 of patients with psychotic dementia show marked distress (Ballard et al., 1995)
Pharmacological Treatment • One third of all atypical antipsychotic prescriptions are written for elderly people in long-term care (Schneider, 2002). • Significant adverse effects reported with atypical antipsychotics (Schneider et al., 2006) • Typicals and atypicals associated with increased short-term mortality in dementia (Triforo et al., 2006) • Risperidone is considered most effective (Fischer et al., 2006) • And patients taking antipsychotics are no more likely to decline cognitively (Livingston et al., 2006).
Pharmacological Treatment • Interestingly, donepezil seems to operate as an effective ‘antipsychotic’ (Cummings et al., 2006) • Again, suggesting a strong link between cognitive decline and psychosis. • Which doesn’t seem to be so apparent in idiopathic psychosis.
Nonpharmacological Treatment • “These results and the evidence that behavioral problems in Alzheimer’s disease can be reduced by specialized care that stresses nonpharmacologic management suggest that these drugs have a limited, but at times necessary, role in the care of patients with Alzheimer’s disease” • Karlawish (2006) • There are many studies, and many approaches, but very little adequately executed research into efficacy (Cohen-Mansfield, 2001)
Nonpharmacological Treatment • A recent review (Ayalon et al., 2006) only included systematic studies of sufficient quality. • A grand total of 3 RCTs and 6 single case studies! • Identified three main approaches for neuropsychiatric symptoms: • Unmet needs (i.e. functional analysis approach) • Learning / behavioural interventions • Environmentalvulnerability / stress threshold • All approaches were deemed “possibly efficacious, pending replication of findings”.
Nonpharmacological Treatment • For delusions specifically, the advice is similar for delusions from idiopathic psychosis (Rabins, 1994): • Reassurance • Distraction • Discussing other matters • Discussing feelings behind the delusion
Conclusions • Delusions present differently in dementia. • They are common, and increase over time. • They are associated with significant distress and behaviour disturbance. • They are strongly associated with cognitive decline. • Pharmacotherapy is moderately effective but risky. • Psychological therapy is less risky, promising, but largely untested.