Download
1 / 32
350 likes | 594 Views
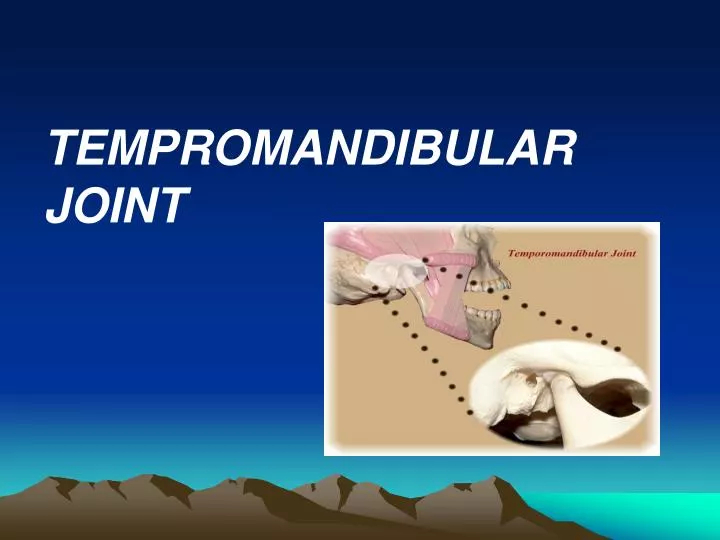
TEMPROMANDIBULAR JOINT. TMJ: is a bilateral joints permits the mandible to move as a unit with two functional patterns: Hinge (inferior portion) Translation (superior portion) (ginglymoarthroidal joint) (compound joint) it has four anatomical parts: 1- condyle

E N D
TEMPROMANDIBULAR JOINT
TMJ: is a bilateral joints permits the mandible to move as a unit with two functional patterns: • Hinge (inferior portion) • Translation (superior portion) (ginglymoarthroidal joint) (compound joint) it has four anatomical parts: 1- condyle 2- articular fossa 3- articular disc 4- articular capsule
The Synovial fluid: Consist of small amounts of a clear, straw-colored viscus fluid. It is an infiltrate of the blood diffused out from the rich capillary network of the synovial membrane. Function: 1- lubrication by two mechanisms: boundry lubrication weeping lubrication 2- nutrition. 3- clear the tissue debris.
Ligaments : 1-collateral(discal) 2-capsular 3-tempromandibular 4-sphenomandibular 5-stylomandibular
Muscles of mastication: 1- masseter: superficial & deep 2- temporalis 3- medial pterygoid 4- lateral pterygoid: superior & inferior - Digastric muscles is not a muscle of mastication but it play an important role in mandibular function.
Nerve supply: the mandibular division of the trigeminal nerve. Vascular supply: superficial temporal artery--- post middle meningeal artery--- ant internal max.artery---- inf deep auricular Anterior tympanic Ascending pharengeal arteries
Control of TMJ movements: -Vertical jaw reflexes: 1-jaw jerk 2-jaw opening 3-jaw unloading -horizontal jaw reflexes
Age changes of theTMJ: 1- Flattened condyle 2- osteoporosis of the condyle bone. 3- Thickning of the fibrous covering of the condyle. 4- Thinning of the cartilagenous zone of condyle. 5- Thinning of the disc 6- Fibrotic synovial folds 7- Thickening of the b.v. walls 8- Decrease the number of nerves
These age changes lead to: -Decrease in the synovial fluid formation -Impairment of motion due to decrease in the disc and capsule extensibility -Decrease the resilience during mastication due to chondroid changes into collagenous elements -Dysfunction in older people
Disorders of the TMJ: 1- limitation of movement: - temporary - permanent 2- dislocation 3- pain 4- hyperplasia 5- neoplasm 6- loose bodies in the TMJ
1-limitation of mandibular movement: due to: a-intracapsular causes: Infective arthritis Juvenile arthritis Traumatic arthritis Intracapsular condyle fracture b-pericapsular causes: Irradiation Dislocation Condylar neck fracture Infection of adjacent tissues
c-muscular: Tmj dysfunction syndrome Myalgia due bruxism Haematoma from ID block Tetanus d-Others: Oral submucous fibrosis Systemic sclerosis Zygomatic & maxillary fracture Drugs Craniofacial anomalies involving the joint
Limitation of TMJ movements: Temporary persistent (trismus) (ankylosis)
1-Temporary (trismus):due to: • infection & inflammation in or near the joint • Injuries • tetanus & tetany • TMJ dysfunction syndrome • drugs • hysterical
2-Dislocation: due to: -blow on the jaw -forceful extraction -while yawning -epileptic pt recurrent dislocation is a typical feature of ehler-danlos & marfan’s syndrome or there may be no systemic disorder.
Types of displacement: 1-anterior disc displacement with reduction: Joint noise, pain, clicking and full range of movements 2-acute anterior disc displacement without reduction: Acute onset of limitation of opening with pain & deviation to the affected side, history of clicking 3-chronic anterior disc displacement without reduction: Limitation of opening for variable period,history of clicking
3-Pain in or around the joint:due to: • injury • infection & inflammation • vascular disease e.g: cranial arteritis • muscle spasm e.g: pain dysfunction syndrome • rheumatoid & other arthritis • salivary gland disease e.g: parotid neoplasm • ear disease e.g: otitis media, externa
4-Hyperplasia: Is rare unilateral overgrowth of the condyle. It causes: facial asymmetry, deviation of the jaw to the unaffected side on opening and crossbite. Treated by: -If it is stabilized at the end of puberty --- corrective osteotomies to restore occlusion & facial asymmetry -If it is still active --- intracapsular condylectomy
5-Neoplasms:(rare): • osteochondroma • osteoma • chondroma
6-Loose bodies in the TMJ: (rare): • osteochondritis disssecans: due to trauma • synovial chodromatosis benign neoplasm
Examination: 1-joint examination: static: palpation x.rays ( tomography) dynamic: mobility limitation sounds 2-muscle examination: palpation movement limitation pain on movements 3-occlusal examination: study cast facebow regestration
Management: Goals: - decreased pain - decreased loading - restored function - restored daily activities
Management options: 1-Pt.education & palliative home care:yawning 2-Behaviour modifications: habits 3-Drug therapy: e.g: NSAID, analgesics 4-Exercise therapy 5-Splint therapy 6-Occlusal therapy 7-mobilization 8-Physical agents: heat,cold,muscle relaxation 9-Other therapy: joint surgery, orthodontics.




![TEMPROMANDIBULAR JOINT AND MOVEMENTS MANDIBULAR [ T M J ]](https://cdn3.slideserve.com/6414015/slide1-dt.jpg)