Download

1 / 25
330 likes | 869 Views
Antidepressant Therapy in the Elderly Population . Johanna Rivera, Pharm.D . Candidate 2014 Sydney Kchao , Pharm.D . Candidate 2014 Preceptor: Joshua Caballero, Pharm.D ., BCPP. Epidemiology 1, 2, 3, 4. Choosing Between Antidepressants 5. P revious response to treatment

E N D
Antidepressant Therapy in the Elderly Population Johanna Rivera, Pharm.D. Candidate 2014 Sydney Kchao, Pharm.D. Candidate 2014 Preceptor: Joshua Caballero, Pharm.D., BCPP
Choosing Between Antidepressants 5 • Previous response to treatment • Type of depression • Comorbidities • Side effect profile • Interactions • Potential risk of overdose • Drug cost to patient • Compliance issues
Initial dose: 5 mg/d • Drug interactions: Minimal • Monitor for QT interval prolongation • Other formulations: • Oral solution (Generic/brand) • Initial dose: 10 mg/d • Drug interactions: Minimal • FDA Warning: Citalopram causes dose-dependent QT interval prolongation. Max dose in patients >60YO should not exceed 20 mg per day • Other formulations: • Oral solution (Generic) 1st Line Selective Serotonin Reuptake Inhibitors (SSRIs)6 • Citalopram (Celexa®) • Escitalopram (Lexapro®)
Activating SSRIs Fluoxetine (Prozac®) Sertraline (Zoloft®) Initial dose: 25 mg/d Alzheimer’s-related depression initial dose: 12.5 mg/d Drug Interactions: CYP2D6 (Potent at doses >200 mg/d), 3A4, 2B6, 2C9, 2C19 (Minor) Other formulations: Oral solution (Generic/brand) • Initial dose: 10 mg/d • Drug Interactions: CYP2D6 (Potent), 2C9, 2C19, 2B6, and 3A4 • Other formulations: • Oral solution & syrup (generic) • 90 mg delayed released capsule taken once per week
Sedating SSRIs7 Paroxetine (Paxil®) Fluvoxamine (Luvox®) Initial dose: 25 mg/d Drug Interactions: CYP2D6, 1A2, 2C19, 3A4 (Potent) Other formulations: ER (Generic/brand) • Initial dose: 10 mg/d • Weak anticholinergic • Drug Interactions: CYP2D6, 2B6 (Potent) • Other formulations: • Oral suspension • ER (Generic/brand)
2nd Line Serotonin NorepinephrineReuptake Inhibitors (SNRIs)8, 9 Venlafaxine (Effexor®) Desvenlafaxine (Pristiq®) Activating Initial dose: 50 mg/d Renal adjustment: CrCl < 30 mL/min 50 mg every other day Drug interactions: Minimal • Activating • Initial dose: 18.75 to 37.5 mg/d • Drug interactions: Weak inhibitor CYP2D6 & 3A4. Major substrate of 2D6 & 3A4 • Duloxetine (Cymbalta®) • Mildly sedating • Initial dose: 10-20 mg/d • Drug interactions: CYP1A2 & 2D6 (Potent)
2nd Line Mirtazapine (Remeron®) 10 • Other formulations: • Rapidly dissolving sol-tab (Generic/brand) • Side effects include: • Sedation appetite increase and weight gain, dry mouth, and constipation • Drug interactions: CYP2D6, 1A2, 3A4 (Potent) • Sedating agent (at initiation and/or lower doses), • Initial Dose: 7.5 mg/d • Useful for elderly patients with insomnia, agitation or restlessness, and anorexia or weight loss • Also useful in patients with Parkinsonism, essential tremor, or nausea from chemotherapy
Bupropion (Wellbutrin®) 11 • Activating agent • Initial dose: 75 mg/d • Useful in patients who complain of lethargy, daytime sedation, or fatigue. • Dopaminergic action may be advantageous for depressed patients with Parkinson disease. • Dose-dependent diastolic hypertension • Contraindicated: • Seizure disorders • Concurrent use of benzo’s or other CNS depressants • Alcohol detoxification • Prior diagnosis of bulimia, anorexia nervosa • Drug Interactions: CYP2D6 (Potent)
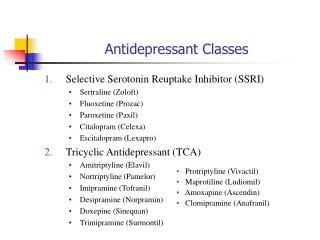
TCAs11 • Tertiary (BEERS CRITERIA AVOID.) • Amitriptyline • Imipramine • Doxepin • Trimipramine • Secondary • Nortriptyline (Pamelor®) • Desipramine (Norpramin®) • Protriptyline (Vivactil®) • Sedating Agents (except Vivactil®) • Anticholinergic effects • Use cautiously in patients with cardiac conduction abnormalities, arrhythmias, narrow angle glaucoma, urinary retention, or BPH. • Patients with Alzheimer-type dementia may experience worsening confusion. • May be fatal in overdose
Monoamine Oxidase Inhibitors (MAOIs) 11 • Tranylcypromine • Phenelzine • Selegiline • Activating agent • Rarely used except when previously initiated and tolerated, or in the patient who is treatment resistant to all other antidepressants • Side effects: orthostatic hypotension and insomnia • Diet restrictions: • Tyramine containing foods: Aged cheeses, aged and cured meats, draft beer, etc. • Drug Interactions: MANY
Switching Between Antidepressants12, 13, 14, 15Cross-Tapering New Antidepressant Current Antidepressant 1 to 2 Week Period or Longer *Clinical Pearl: When prescribing two antidepressants, state on the prescription that you are cross-tapering.
SSRI to SSRI New SSRI Current SSRI Current SSRI New SSRI
SSRI to TCA New TCA Current SSRI • 1 to 2 Week Period or Longer • SSRIs can inhibit hepatic enzymes that metabolize TCAs • Most SSRIs are cleared in 5 days (exception: 5 weeks for fluoxetine) • Serum TCA concentrations can be checked for safety
SSRI to Venlafaxine or Duloxetine Current SSRI Venlafaxine or Duloxetine • If current SSRI is high dose, consider cross taper • Caution when switching from fluoxetine and paroxetine due to 2D6 inhibition, start with low dose Venlafaxine or Duloxetine
Venlafaxine or Duloxetine to other Antidepressant other than MAOIs Venlafaxine or Duloxetine Antidepressant other than MAOIs • 2 to 3 Week Period or Longer • Venlafaxine is associated with uncomfortable discontinuation symptoms
Switching Between Venlafaxine & Duloxetine Venlafaxine Duloxetine • Low dose substitution usually well-tolerated • Consider cross-taper at high doses i.e. Venlafaxine >150mg or Duloxetine >60mg
Switching to or from Mirtazapine16 SSRIs TCAs Venlafaxine Duloxetine Mirtazapine • 1 to 2 Week Period or Longer • Cross-taper recommended
Switching to or from Bupropion SSRIs TCAs Venlafaxine Duloxetine Mirtazapine Bupropion • 1 to 2 Week Period or Longer • Bupropion does not have serotonergic properties, so would not be expected to mitigate discontinuation symptoms from medications that are highly serotonergic • CYP 2D6 DDIs – Risk of Seizure with coadministeringBupropion with Fluoxoetine/Paroxetine/Fluvoxamine
Switching to or from MAOIs SSRIs TCAs Venlafaxine Duloxetine Mirtazapine MAOIs • 2 Week Period or Longer • Do not coadminister MAOIs with other antidepressants due to severe toxicity (hypertensive crisis & serotonin syndrome) • Allow two weeks for other antidepressants to wash out before starting MAOI as well (exception: 5 weeks for fluoxetine)
Discontinuation of Antidepressants • Adverse effects when abruptly discontinued • Symptoms can be prevented if patients are informed about risks • Reduce dose about 25% per week over 2-4 weeks • Symptoms for SSRIs may be associated with half-life • Patients with difficulty tapering off of paroxetine may benefit from being switched to an equivalent dose of fluoxetine and then tapering of fluoxetine • Patients who suffer from discontinuation syndrome after an SSRI can be acutely treated with fluoxetine 10 to 20mg per day
Take Home Points & Recommendations • For older adults start at ½ the usual starting dose • First Line: SSRIs • Second Line: Venlafaxine or Duloxetine which are also useful in patients with depression and neuropathic pain. • Mirtazapine useful for patients with insomnia, agitation, restlessness, anorexia, or weight loss. • Third/Fourth Line: TCAs • Resistant Depression: MAOIs • For many drug switches, cross-tapering is the best technique • Allow two weeks before and after using an MAOI with any other antidepressant with exception to fluoxetine (5 weeks) • Fluoxetine persists in the system up to 5 weeks, most SSRIs up to 5 days • Educate patients about discontinuation symptoms
Questions Betty White's Off Their Rockers. N.d. Photograph. z94.com. Web. 24 Jul 2013. <http://wac.450f.edgecastcdn.net/80450F/z94.com/files/2012/04/Betty_WHites_Off_Their_Rockers.png>.
References • Lebowitz BD, Pearson JL, Schneider LS, Reynolds CF, et al. Diagnosis and treatment of depression in late life. Consensus statement update. JAMA. 1997; 278(14): 1186-90. • Steffens DC, Skoog I, Norton MC, Hart AD, et al. Prevalence of depression and its treatment in an elderly population: the Cache County study. Arch Gen Psychiatry. 2000; 57(6): 601-7. • Birrer, RB, Vemuri, SP. Depression in later life: a diagnostic and therapeutic challenge. Am Fam Physician 2004; 69: 2375. • Percentage of Suicides, by Age Group, Sex and Mechanism, United States, 2005–2009. Centers for Disease Control and Prevention.2012. Retrieved July 23, 2013, from http://www.cdc.gov/violenceprevention/suicide/statistics/mechanism02.html • Wiese BS. Geriatric depression: The use of antidepressants in the elderly. BCMJ. 2011; 53(7): 341-347. Retrieved July 21, 2013, from http://www.bcmj.org/articles/geriatric-depression-use-antidepressants-elderly • Kok RM,HeerenTJ, Nolen WA, PhD. Continuing Treatment of Depression in the Elderly: A Systematic Review and Meta-Analysis of Double-Blinded Randomized Controlled Trials With Antidepressants. The American Journal of Geriatric Psychiatry. 2011; 19(3): 249. • Flockhart DA. Drug Interactions: Cytochrome P450 Drug Interaction Table. Indiana University School of Medicine. 2007. Retrieved July 22, 2013, from "http://medicine.iupui.edu/clinpharm/ddis/clinical-table • Nelson JC, Wohlreich MM, Mallinckrodt CH,et al. Duloxetinefor the treatment of major depressive disorder in older patients. Am J GeriatrPsychiatry 2005; 13(3): 227.
References 9. OslinDW, Ten Have TR, Streim JE, et al. Probing the Safety of Medications in the Frail Elderly: Evidence from a Randomized Clinical Trial of Sertraline and Venlafaxine in Depressed Nursing Home Residents. J Clin Psychiatry. 2003; 64(8): 875. 10. Nelson JC, Holden K, Roose S, et al.International Journal of Geriatric Psychiatry. 2007; 22(10): 999-1003. 11. Facts & Comparisons eAnswers [online]. 2013.WoltersKluwer Health, Inc. Accessed July 24, 2013. 12. Warner CH, Bobo W, Warner C, et al. Antidepressant discontinuation syndrome. Am Fam Physician 2006; 74: 449. 13. Rosenbaum JF, Zajecka J. Clinical management of antidepressant discontinuation. J Clin Psychiatry 1997; 58(7): 37. Tint A, Haddad PM, Anderson IM. The effect of rate of antidepressant tapering on the incidence of discontinuation symptoms: a randomized study. J Psychopharmacol2008; 22: 330. Ogle NR, Akkerman SR. Guidance for the Discontinuation or Switching of Antidepressant Therapies in Adults. J PharmPract2013; 1: 8. 16. KlesmerJ, Sarcevic A, Fomari V. Panic attacks during discontinuation of mirtazepine. Can J Psychiatry 2000; 45: 570.