Download
1 / 29
1.02k likes | 3.73k Views
PELD (Percutaneous Endoscopic Lumbar Discectomy). Spine center / Chung-Mu Hospital. 1. History of PELD. Hijikata 1977 ; Percut. discectomy Kambin 1983 ; Percut. lateral discectomy ( AMD ) Onik 1985 ; Automated percut. lumbar discectomy ( APLD )

E N D
PELD (Percutaneous Endoscopic Lumbar Discectomy) Spine center / Chung-Mu Hospital
Hijikata 1977 ; Percut. discectomy • Kambin 1983 ; Percut. lateral discectomy ( AMD ) • Onik 1985 ; Automated percut. lumbar discectomy ( APLD ) • Schreiber 1986 ; Transdiscoscopic percut. nucleotomy • Mayer 1989 ; Percut. endoscopic lumbar discectomy • Lee 1992 ; Percut. endoscopic mechanical & • laser discectomy
Transforaminal Lumbar Discectomy Hallett Mathews (1996) ; Neurosurgery David A. Ditsworth (1998) ; Surgical Neurology
Current status of Percutaneous Discectomy Mechanical removal of disc matrial & laser thermal modulation under endoscopic control. • Kambin • Schreiber and Leu • Mayer and Brock • Bonati • Siebert • Savitz • Yeung • Chiu • Knight
Review of several reports about surgical Tx on L1-2 disc herniation • Post. Laminectomy and discectomy • Anterolateral discectomy and fusion
Dilemmas of surgical Tx. • How to avoid excessive neural retraction ? • How to avoid unnecessary bone fusion ?
PELD as an alternative ! • Direct access to the lesion without • unwanted tissue damage • Can avoid neural retraction • Can avoid bone fusion
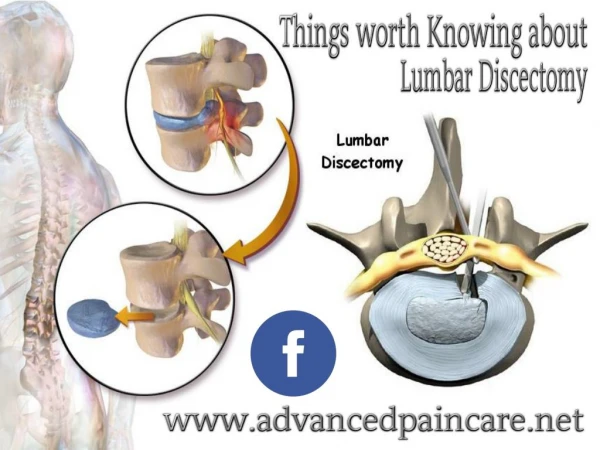
The Aim of Percutaneous Discectomy • Not to decrease the intradiscal pressure • But to remove the herniated fragment itself (Herniotomy)
Advantages Protection of epidural and neural venous systems and prevention of venous stasis and chronic neural edema. Prevention of epidural bleeding and subsequent development of perineural and epidural scar formation. Protection of fine dural and neural ligamentous structures. Prevention of injury and denervation of paraspinal muscles. Protection against the development of post surgical instability due to excessive bone or facet removal. Minimizing the incidence of recurrent disc herniation by protection of posterior annular fiber and PLL. Being an access of choice for foraminal and extraforaminal herniations without facet resection. Treat LBP also.
Disadvantages The difficulties associated with the migrated sequestrated disc fragments. Access to L5-S1 intervertebral disc at the presence of elevated iliac crest. Stenosis.
Radiologic Indications Migrated but not sequestrated herniation Foraminal & extraforaminal herniation Recurrent herniation No stenosis, no instability, and no collapse of disc height
Contraindications A calcified disc herniation and severe degenerative changes of facet. relative contraindications. Aspirin and other pain medications which may produce coagulopathy must be avoided before surgery. Instability.
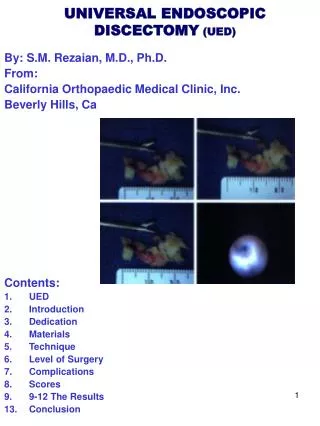
IV sedation under local anesthesia 18G needle insertion Discography (Indigocarmine + dye) Guide wire insertion Cannula insertion Annulotomy Forceps & laser with endoscope
How to reach herniated fragments The forceps should reach subligamentously beyond the posterior body line.
Technical Evolution Safe zone app. Transforaminal app. Intradiscal app. Subligamentous app. Epidural endoscope
7. Conclusion The percutaneous endoscopic transforaminal laser-assisted Lumbar discectomy is useful in treating extruded lumbar disc Herniation with minimal migration.