Download
1 / 102
1.06k likes | 1.82k Views
Head and Spinal Cord Trauma. May 2011 CE Condell Medical Center EMS System Site Code #107200E-1211 Objectives by: Mike Higgins, FF/PM Grayslake Fire Department Packet by: Sharon Hopkins, RN, BSN, EMT-P. Objectives.

E N D
Head and Spinal Cord Trauma May 2011 CE Condell Medical Center EMS System Site Code #107200E-1211 Objectives by: Mike Higgins, FF/PM Grayslake Fire Department Packet by: Sharon Hopkins, RN, BSN, EMT-P
Objectives • Upon successful completion of this module, the EMS provider will be able to: • List risky behaviors contributing to brain and spinal cord injuries. • Describe typical injury patterns related to specific mechanisms of injury. 3. Describe the anatomy of the brain. 4. List contents of the skull. 5. Describe the mechanisms for the development of secondary brain injury. 6. Describe the pathophysiology of traumatic brain injuries including pressures related to brain blood flow. 7. Explain the normal anatomy and physiology of the spinal column and spinal cord.
Objectives cont’d 8. Describe the pathophysiology of traumatic spinal cord injuries. 9. Describe components of a neurological assessment in the field. 10. List signs and symptoms of spinal cord injuries. 11. Describe the pathophysiology of neurogenic shock. 12. Describe prehospital treatment based on Region X SOP’s of the patient with a head or spinal cord injury. 13. Review ventilation rates of the stable and unstable patients with head and/or spinal cord injuries.
Objectives cont’d 14. Review the Region X Infield Spinal Clearance SOP. 15. Review measurement of fitting a cervical collar. 16. Review the procedure for demonstrating the standing backboard takedown procedure. 17. Demonstrate the proper measurement and placement of a cervical collar. 18. Demonstrate the standing take down with the back board. 19. Actively participate in case scenario discussion. 20. Successfully complete the post quiz with a score of 80% or better.
What’s The Big Deal? • Traumatic brain injury (TBI) • Major cause of death and disability in multiple trauma patients • Severe injury indicated with GCS <9
TBI Statistics • Many patients will be minors, therefore, you will also be dealing with parents and caregivers
Traumatic Brain Injury (TBI) • 40% of trauma patients have CNS injury • Death rate twice as high (35%) as patient without CNS injury • Account for 25% of all trauma deaths • Account for up to 50% of all MVC deaths • Cost worldwide is huge • Lives lost • Families destroyed • Money spent for care CNS – central nervous system
Risky Activities Resulting in Spinal Cord Injuries • MVC – 44.5% - major cause • SUV’s & jeeps prone to flipping • Falls 18.1% • Most common in persons >45 years of age • Violence 16.6% • More common in urban settings • Sports 12.7% • Diving most common contributing sport • Other medical causes make up <10%
Typical Head/Neck Injury Patterns • T-bone – lateral impact • Coup/contrecoup head injuries • Neck strain up to fractures • Most injuries from collision with inside of vehicle • Rear impact • Hyperextension of neck esp if head rest not fitted • Lumbar spine injury if seat breaks • Rollover • Body impacted in all directions so injury potential high • Increased chance for axial loading on spine • Often lethal injuries when ejected
Typical Head/Neck Injury Patterns • ATV • Injuries depend on MOI and part of body impacted • High index of suspicions for head and spinal injuries • Falls from height • Evaluate distance, body area impacted, type of surface struck • Landing on feet, check for axial loading to lumbar and cervical spine areas
Anatomy of the Skull • Scalp highly vascular • Skull is rigid bone • Serves as protection • Dura mater • Tough fibrous covering of brain • Arachnoid mater • Lies under dura • Arteries & veins suspended from this • Pia mater • On surface of brain
Anatomy of the Brain • Each lobe has a unique function • Identified disabilities can help pinpoint area of insult or injury • Proper assessment can point to area of injury • Always reassess watching for trends
Anatomy of the Brain • Cerebrum • Frontal lobe • Personality • Judgment • Temporal lobe • Hearing • Memory • Parietal lobe • Language formation; processing senses • Occipital lobe • Vision
Anatomy cont’d • Cerebellum • Control of movement, balance, coordination • Brainstem • arousal & consciousness center; involved in basic life functions • breathing, reflexes • Pons – motor & sensory relay center • Medulla- controls autonomic functions (breathing, digestion, heart & blood vessel function
Contents of the Skull • There is no extra space • If one component increases, usually brain tissue swelling, it is usually at sacrifice of one of the other components • Brain – 80% • Blood volume – 10% (150 ml) • CSF – 10% (150 ml ) CSF – cerebral spinal fluid
Brain Function • Brain VERY sensitive to levels of oxygen and glucose • Brain has a high metabolic rate both at rest or engaged in activity • Brain is 2% of total body weight • Receives 15% of cardiac output • Consumes 20% of body’s oxygen • Relies on aerobic metabolism • Needs constant availability of glucose, thiamine (to metabolize glucose), and oxygen
Adding Insult to Injury • Coup-contrecoup injuries • Brain shifts/floats inside skull • Base of skull rough – causes more injury • Injuries at point of impact and away from point of impact • Ex: forehead injury can result in additional injury to occipital area
Secondary Injury • Primary injury occurs at time of insult • Secondary injury occurs later as a result of what happens initially • Initial swelling causes decreased perfusion • Secondary complications stem from hypoxia and decreased perfusion
What is your major focus? • Management of injury focused on • Proper care • Identification of injuries • An accurate general impression leads to appropriate care • Appropriate interventions initiated • Rapid transport to secondary care • Do things right to prevent contributing to secondary injuries
Common Problems Related To TBI • Airway compromise • Inadequate ventilation • Hypotension • An independent risk factor contributing to mortality • Focus on these critical aspects and perform appropriate interventions as needed
Pressures Related to Blood flow • ICP is pressure of brain and contents within skull • CPP - cerebral perfusion pressure • Pressure of blood flowing thru brain; pressure necessary to perfuse brain (CPP=MAP-ICP) • MAP - mean arterial pressure • Average pressure within an artery; pressure maintained in vascular system
Reflexive Response to ICP • Cushing’s reflex • Protective response to preserve blood flow to the brain • B/P will increase • Systolic B/P increasing as diastolic B/P stays same or increases • Widening pulse pressure • Heart rate will decrease • Effort to lower elevating blood pressure • Respirations may be irregular • Note vital signs move opposite to shock
Cerebral Perfusion • Brain requires unique range to function • Increased ICP causes brain herniation • Hypotension not tolerated with ICP • Examples of problems*: • MAP constant + ICP = CPP • MAP decreases + ICP steady = CPP • MAP decreases + ICP = CPP critical • Any negative change in B/P or ICP affects blood flow in brain • *Normal values of MAP, ICP, and CPP listed in Notes section
Signs and Symptoms Head Injury • Use inspection/observational skills with mechanism of injury to increase suspicion of head and neck injuries
Brain Injuries - Concussion • Prevalent in athletic activities • No structural injury to brain • Often brief loss of consciousness or, at minimum, confusion, then return to normal • Possible amnesia (short-term retrograde) • Short term memory loss – will ask repetitive questions • Dizziness, headache, ringing in ears, nausea
Brain Injuries – Cerebral Contusion • Bruised brain tissue • History prolonged unconsciousness or serious altered level of consciousness (confusion, amnesia, abnormal behavior) • Focal neurological signs • Related to a specific area of the brain • Weakness, speech problems, personality or behavioral changes
Brain Injuries – Subarachnoid Hemorrhage • Blood in subarachnoid space • Traumatic injury or spontaneous • Blood causes irritation • Severe headache • “Worst headache of my life” • Coma • Vomiting
Brain Injuries – Diffuse Axonal Injury • Most common type of injury from blunt head trauma • Generalized, diffuse edema • Unconscious • No focal deficits • Swelling, edema, injury too widespread so no specific isolated sign/symptom pointing to 1 area of the brain
Brain Injuries – Acute Epidural Hematoma • Bleeding between dura and skull • Often from tear in middle meningeal artery from skull fracture in temporal area • Runs along inside of skull in temporal area • Arterial bleed so onset usually rapid for signs/symptoms • Initial loss of consciousness and now lucid • Signs ICP after few hours • Vomiting, headache, altered mental status • Motor deficit opposite side to injury (contralateral) • Dilated, fixed pupil on side of injury (ipsilateral)
Brain Injuries – Acute Subdural Hematoma • Bleeding between dura and arachnoid • Bleeding is venous • Slow onset to ICP (hours, days) • Headache, changing level of consciousness, focal neurological signs • Weakness one sided, slurred speech • Poor prognosis due to associated brain tissue injury • High risk: elderly, anticoagulant use, chronic alcoholics
Brain Injuries – Intracerebral Hemorrhage • Bleeding within brain tissue • Blunt or penetrating injuries • Surgery not often helpful • Signs and symptoms depend on region of brain injured • Patterns similar to a patient with a stroke • Altered level of consciousness common • If awake, complain of headache & vomiting
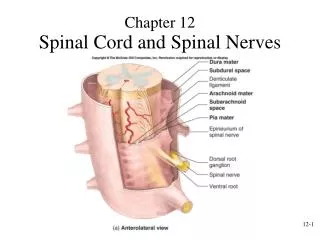
Spinal Column • Spinal column is the bony tube of 33 vertebrae separated by discs that act as shock absorbers • Alignment maintained by strong ligaments and muscles • Supports body in upright position • Allows use of extremities • Protects delicate spinal cord
Spinal Cord • Electrical conduit • Extension of brain stem • Continues down to first lumbar vertebrae then separates into nerves • Surrounded and bathed by cerebrospinal fluid • Cerebrospinal fluid and flexibility provide some protection
Spinal Cord cont’d • Nerve roots exit at each vertebral level • Nerve roots carry signals from brain to specific sites • Nerve roots carry sensory signals from body to spinal cord to brain • Susceptible to traumatic injury
Spinal Cord cont’d • Integrates/brings together the autonomic nervous system • 2 components: parasympathetic and sympathetic nervous system • Assists in controlling • Heart rate • Blood vessel tone • Blood flow to skin
Mechanisms of Injury • Penetrating injuries • Secure the object in position found • Do no further harm!
Mechanisms of Blunt Spinal Injury • Hyperextension • Excessive posterior movement of head or neck • Face into windshield • Elderly person falling to floor, striking chin • Football tackler • Dive into shallow water • Hyperflexion • Excessive anterior movement of head onto chest • Rider thrown from horse or motorcycle • Dive into shallow water
Mechanisms cont’d • Compression • Weight of head or pelvis driven into stationary neck or torso • Dive into shallow water • Fall onto head or legs >10-20 feet • Rotation • Excessive rotation of torso or head & neck; moves one side of spinal column against other side • Rollover MVC • Motorcycle crash
Mechanism cont’d • Lateral stress • Direct lateral force on spinal column; typical shearing one level of cord from another • T-bone MVC • Distraction • Excessive stretching of column and cord • Hanging • Child inappropriately wearing shoulder belt around neck • “Clothes lining” with snowmobile or motorcycle riders and passengers
Disk Problems • A preexisting problem can be aggravated at time of injury
Spinal Cord Injuries • Complete injury • No function, sensation, voluntary movement below level of injury • Both sides affected equally • Incomplete injury • Some function preserved below level of injury • May move 1 limb more than other • May have more function on 1 side of body than other • May have sensation but no movement
Spinal Cord Injuries • Tetraplegia (also referred to as quadriplegia) • Injury in cervical area • Loss of muscle strength in all 4 extremities • Paraplegia • Injury in spinal cord in thoracic, lumbar or sacral segments • Level of impairment dependent on level of injury
Spinal Cord Injury Patterns • Cervical area injury = quadriplegic • C1-C2 – may lose involuntary function of breathing • Watch for excessive use of abdominal muscles to breath • C4 and above – often require use of ventilator for breathing • C5 – shoulder/bicep control but no control of hand or wrist • C6 – wrist control but no hand function
Spinal Cord Injury Patterns • C7-T1 – can straighten arms, dexterity problem with fingers and hands • Thoracic level and below = paraplegic • T1-T8 – has control of hands, poor trunk control due to lack of abdominal muscle control • T9-T12 – good trunk & abdominal muscle control; sitting balance good. Decreased control hip flexor and legs
Spinal Cord Injury Consequences • Often experience: • Bowel and bladder dysfunction • Male fertility often affected • Inability to regulate B/P; hypotension usual • Inability to sweat below level of injury • Decrease control to regulate body temperature • Chronic pain
Dermatomes • Mapping of body • Easier to identify injured areas by isolating location of complaints as related to zones of altered sensation
Neurogenic Shock • Occurs when brain signals interrupted for autonomic functions • Ability to vasoconstrict limited • No sympathetic tone, vessels dilate • Relative hypovolemia • preload ventricular filling Frank Starling reflex contraction strength cardiac output • No hormone release to heart rate
Neurogenic Shock • Signs and symptoms • Bradycardia • Hypotension • Cool, moist, pale skin above cord injury • Warm, dry, flushed skin below cord injury