Download
1 / 1
10 likes | 256 Views
SOMATIZATION IN AN INPATIENT POPULATION. Barbosa F 1 , Sousa F 1 , Ferro A 1 , Santos AL 1 , Lé P 1 , Cardoso D 1 , Mano S 1 , Barbosa A 1,2 1 University Hospital of Santa Maria 2 Faculty of Medicine, University of Lisbon. Introduction. Instruments.

E N D
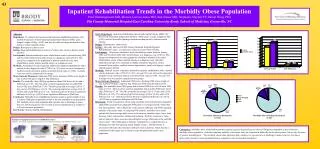
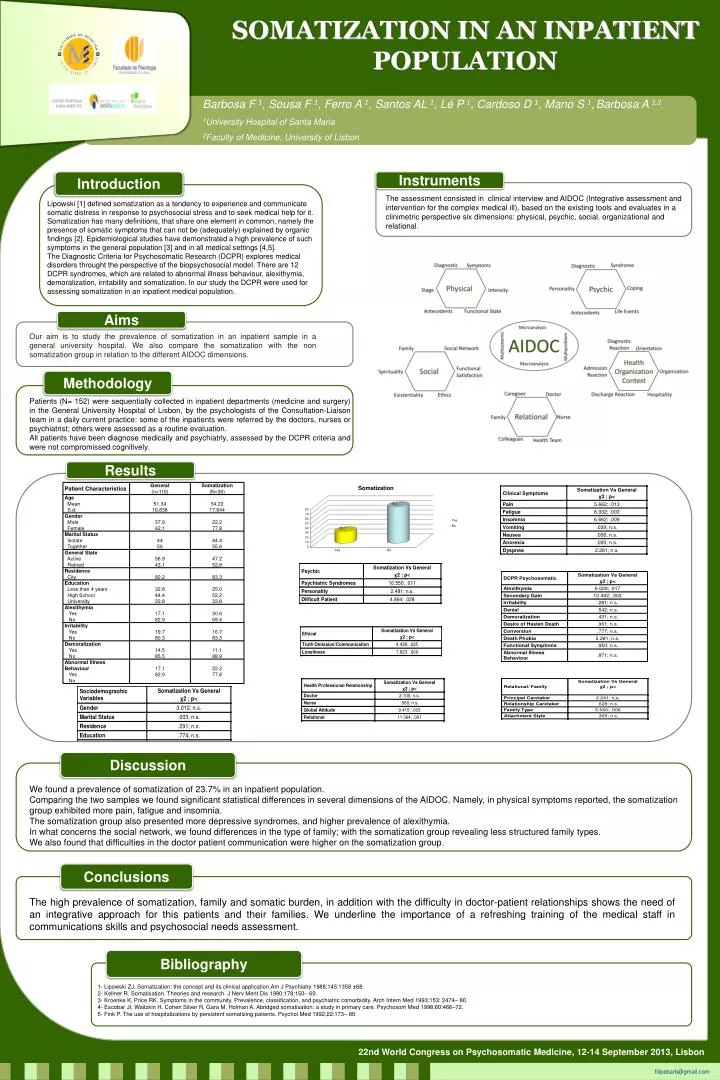
SOMATIZATION IN AN INPATIENT POPULATION Barbosa F 1, Sousa F 1, Ferro A 1, Santos AL 1, Lé P 1, Cardoso D 1, Mano S 1,Barbosa A 1,2 1University Hospital of Santa Maria 2Faculty of Medicine, University of Lisbon Introduction Instruments The assessment consisted in clinical interview and AIDOC (Integrative assessment and intervention for the complex medical ill), based on the existing tools and evaluates in a clinimetric perspective six dimensions: physical, psychic, social, organizational and relational. Lipowski [1] defined somatization as a tendency to experience and communicate somatic distress in response to psychosocial stress and to seek medical help for it. Somatization has many definitions, that share one element in common, namely the presence of somatic symptoms that can not be (adequately) explained by organic findings [2]. Epidemiological studies have demonstrated a high prevalence of such symptoms in the general population [3] and in allmedical settings [4,5]. TheDiagnosticCriteria for PsychosomaticResearch (DCPR) explores medical disordersthroughtthe perspective ofthebiopsychosocialmodel. There are 12 DCPR syndromes, which are related to abnormal illnessbehaviour, alexithymia, demoralization, irritabilityandsomatization. In ourstudythe DCPR wereused for assessingsomatization in aninpatient medical population. Aims Ouraimis to studytheprevalenceofsomatizationinaninpatientsamplein a general university hospital. Wealso compare thesomatizationwiththe non somatizationgroupinrelation to thedifferent AIDOC dimensions. Methodology Patients (N= 152) were sequentially collected in inpatient departments (medicine and surgery) in the General University Hospital of Lisbon, by the psychologists of the Consultation-Liaison team in a daily current practice: some of the inpatients were referred by the doctors, nurses or psychiatrist; others were assessed as a routine evaluation. All patients have been diagnose medically and psychiatrly, assessedbythe DCPR criteriaandwerenotcompromissedcognitively. Results Discussion We found a prevalence of somatization of 23.7% in an inpatient population. Comparing the two samples we found significant statistical differences in several dimensions of the AIDOC. Namely, in physical symptoms reported, the somatization group exhibited more pain, fatigue and insomnia. The somatization group also presented more depressive syndromes, and higher prevalence of alexithymia. In what concerns the social network, we found differences in the type of family; with the somatization group revealing less structured family types. We also found that difficulties in the doctor patient communication were higher on the somatization group. Conclusions The high prevalence of somatization, family and somatic burden, in addition with the difficulty in doctor-patient relationships shows the need of an integrative approach for this patients and their families. We underline the importance of a refreshing training of the medical staff in communications skills and psychosocial needs assessment. Bibliography 1- Lipowski ZJ. Somatization: the concept and its clinical application.Am J Psychiatry 1988;145:1358 ±68. 2- Kellner R. Somatisation. Theories and research. J NervMent Dis 1990;178:150– 60. 3- Kroenke K, Price RK. Symptoms in the community. Prevalence, classification, and psychiatric comorbidity. Arch Intern Med 1993;153: 2474– 80. 4- Escobar JI, Waitzkin H, Cohen Silver R, Gara M, Holman A. Abridged somatisation: a study in primary care. Psychosom Med 1998;60:466–72. 5- Fink P. The use of hospitalizations by persistent somatizing patients. Psychol Med 1992;22:173– 80. 22nd World Congress on Psychosomatic Medicine, 12-14 September 2013, Lisbon filipebarb@gmail.com