Download
1 / 1
10 likes | 254 Views
Introduction Bladder cancer (BCa): 4 th most common cancer in men & 9 th leading cause of death worldwide cystoscopy & urine cytology: current gold standards for diagnosis & surveillance of BCa no ideal tumor marker for non-invasive diagnostic & surveillance at the moment

E N D
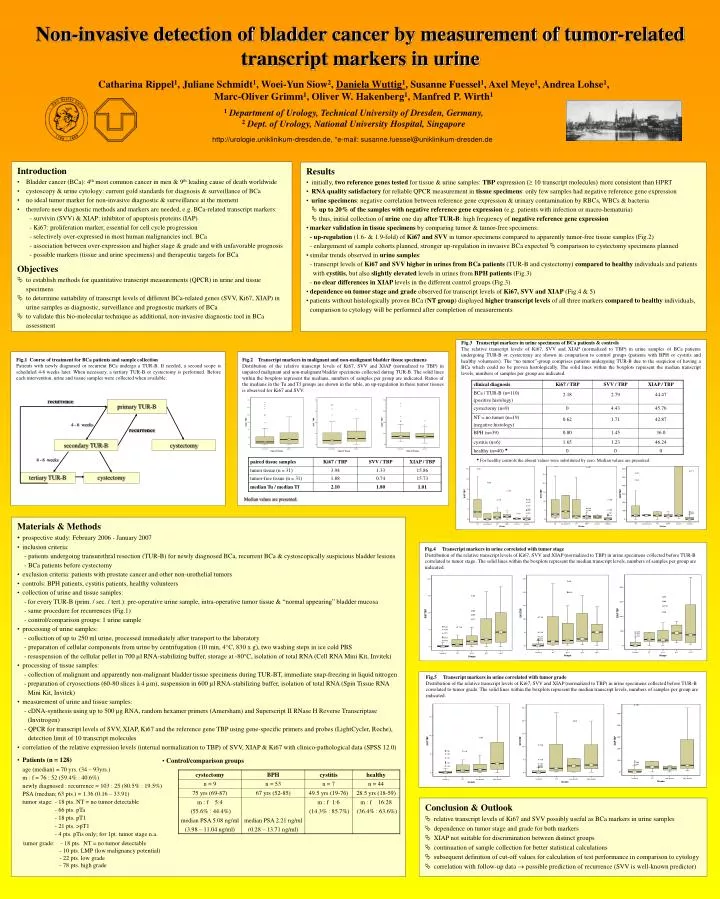
Introduction • Bladder cancer (BCa): 4th most common cancer in men & 9th leading cause of death worldwide • cystoscopy & urine cytology: current gold standards for diagnosis & surveillance of BCa • no ideal tumor marker for non-invasive diagnostic & surveillance at the moment • therefore new diagnostic methods and markers are needed, e.g. BCa-related transcript markers: • - survivin (SVV) & XIAP: inhibitor of apoptosis proteins (IAP) • - Ki67: proliferation marker, essential for cell cycle progression • - selectively over-expressed in most human malignancies incl. BCa • - association between over-expression and higher stage & grade and with unfavorable prognosis • - possible markers (tissue and urine specimens) and therapeutic targets for BCa • Objectives • to establish methods for quantitative transcript measurements (QPCR) in urine and tissue specimens • to determine suitability of transcript levels of different BCa-related genes (SVV, Ki67, XIAP) in urine samples as diagnostic, surveillance and prognostic markers of BCa • to validate this bio-molecular technique as additional, non-invasive diagnostic tool in BCa assessment • Results • initially, two reference genes tested for tissue & urine samples: TBP expression (≥ 10 transcript molecules) more consistent than HPRT • RNA quality satisfactory for reliable QPCR measurement in tissue specimens: only few samples had negative reference gene expression • urine specimens: negative correlation between reference gene expression & urinary contamination by RBCs, WBCs & bacteria • up to 20% of the samples with negative reference gene expression (e.g. patients with infection or macro-hematuria) • thus, initial collection of urine one day after TUR-B: high frequency of negative reference gene expression • marker validationin tissue specimens by comparing tumor & tumor-free specimens: • - up-regulation (1.6- & 1.9-fold) of Ki67and SVV in tumor specimens compared to apparently tumor-free tissue samples (Fig.2) • - enlargement of sample cohorts planned, stronger up-regulation in invasive BCa expected comparison to cystectomy specimens planned • similar trends observed in urine samples: • - transcript levels of Ki67 and SVV higher in urines from BCa patients (TUR-B and cystectomy) compared to healthy individuals and patients • with cystitis, but also slightly elevated levels in urines from BPH patients (Fig.3) • - no clear differences in XIAP levels in the different control groups (Fig.3) • dependence on tumor stage and grade observed for transcript levels of Ki67, SVV and XIAP (Fig.4 & 5) • patients without histologically proven BCa (NT group) displayed higher transcript levels of all three markers compared to healthy individuals, comparison to cytology will be performed after completion of measurements Fig.2 Transcript markers in malignant and non-malignant bladder tissue specimens Distribution of the relative transcript levels of Ki67, SVV and XIAP (normalized to TBP) in unpaired malignant and non-malignant bladder specimens collected during TUR-B. The solid lines within the boxplots represent the medians, numbers of samples per group are indicated. Ratios of the medians in the Tu and Tf groups are shown in the table, an up-regulation in these tumor tissues is observed for Ki67 and SVV. Fig.3 Transcript markers in urine specimens of BCa patients & controls The relative transcript levels of Ki67, SVV and XIAP (normalized to TBP) in urine samples of BCa patients undergoing TUR-B or cystectomy are shown in comparison to control groups (patients with BPH or cystitis and healthy volunteers). The “no tumor”-group comprises patients undergoing TUR-B due to the suspicion of having a BCa which could no be proven histologically. The solid lines within the boxplots represent the median transcript levels, numbers of samples per group are indicated. recurrence primary TUR-B Fig.1 Course of treatment for BCa patients and sample collection Patients with newly diagnosed or recurrent BCa undergo a TUR-B. If needed, a second scope is scheduled 4-6 weeks later. When necessary, a tertiary TUR-B or cystectomy is performed. Before each intervention, urine and tissue samples were collected when available. 4 - 6 weeks recurrence secondary TUR-B cystectomy 4 - 6 weeks tertiary TUR-B cystectomy For healthy controls the absent values were substituted by zero. Median values are presented. Median values are presented. • Materials & Methods • prospective study: February 2006 - January 2007 • inclusion criteria: • - patients undergoing transurethral resection (TUR-B) for newly diagnosed BCa, recurrent BCa & cystoscopically suspicious bladder lesions • - BCa patients before cystectomy • exclusion criteria: patients with prostate cancer and other non-urothelial tumors • controls: BPH patients, cystitis patients, healthy volunteers • collection of urine and tissue samples: • for every TUR-B (prim. / sec. / tert.): pre-operative urine sample, intra-operative tumor tissue & “normal appearing” bladder mucosa • - same procedure for recurrences (Fig.1) • - control/comparison groups: 1 urine sample • processing of urine samples: • - collection of up to 250 ml urine, processed immediately after transport to the laboratory • - preparation of cellular components from urine by centrifugation (10 min, 4°C, 830 x g), two washing steps in ice cold PBS • resuspension of the cellular pellet in 700 µl RNA-stabilizing buffer, storage at -80°C, isolation of total RNA (Cell RNA Mini Kit, Invitek) • processing of tissue samples: • - collection of malignant and apparently non-malignant bladder tissue specimens during TUR-BT, immediate snap-freezing in liquid nitrogen • preparation of cryosections (60-80 slices à 4 µm), suspension in 600 µl RNA-stabilizing buffer, isolation of total RNA (Spin Tissue RNA Mini Kit, Invitek) • measurement of urine and tissue samples: • - cDNA-synthesis using up to 500 µg RNA, random hexamer primers (Amersham) and Superscript II RNase H Reverse Transcriptase (Invitrogen) • - QPCR for transcript levels of SVV, XIAP, Ki67 and the reference gene TBP using gene-specific primers and probes (LightCycler, Roche), detection limit of 10 transcript molecules • correlation of the relative expression levels (internal normalization to TBP) of SVV, XIAP & Ki67 with clinico-pathological data (SPSS 12.0) • Patients (n = 128) • age (median) = 70 yrs. (34 – 93yrs.) • m : f = 76 : 52 (59.4% : 40.6%) • newly diagnosed : recurrence = 103 : 25 (80.5% : 19.5%) • PSA (median; 63 pts.) = 1.36 (0.16 – 33.91) • tumor stage: - 18 pts. NT = no tumor detectable • - 66 pts. pTa • - 18 pts. pT1 • - 21 pts. >pT1 • - 4 pts. pTis only; for 1pt. tumor stage n.a. • tumor grade: - 18 pts. NT = no tumor detectable • - 10 pts. LMP (low malignancy potential) • - 22 pts. low grade • - 78 pts. high grade Fig.4 Transcript markers in urine correlated with tumor stage Distribution of the relative transcript levels of Ki67, SVV and XIAP (normalized to TBP) in urine specimens collected before TUR-B correlated to tumor stage. The solid lines within the boxplots represent the median transcript levels, numbers of samples per group are indicated. Fig.5 Transcript markers in urine correlated with tumor grade Distribution of the relative transcript levels of Ki67, SVV and XIAP (normalized to TBP) in urine specimens collected before TUR-B correlated to tumor grade. The solid lines within the boxplots represent the median transcript levels, numbers of samples per group are indicated. • Control/comparison groups • Conclusion & Outlook • relative transcript levels of Ki67 and SVV possibly useful as BCa markers in urine samples • dependence on tumor stage and grade for both markers • XIAP not suitable for discrimination between distinct groups • continuation of sample collection for better statistical calculations • subsequent definition of cut-off values for calculation of test performance in comparison to cytology • correlation with follow-up data possible prediction of recurrence (SVV is well-known predictor) Non-invasive detection of bladder cancer by measurement of tumor-related transcript markers in urine Catharina Rippel1, Juliane Schmidt1, Woei-Yun Siow2, Daniela Wuttig1, Susanne Fuessel1, Axel Meye1, Andrea Lohse1, Marc-Oliver Grimm1, Oliver W. Hakenberg1, Manfred P. Wirth1 1 Department of Urology, Technical University of Dresden, Germany, 2 Dept. of Urology, National University Hospital, Singapore http://urologie.uniklinikum-dresden.de, *e-mail: susanne.fuessel@uniklinikum-dresden.de