Download
1 / 18
180 likes | 438 Views
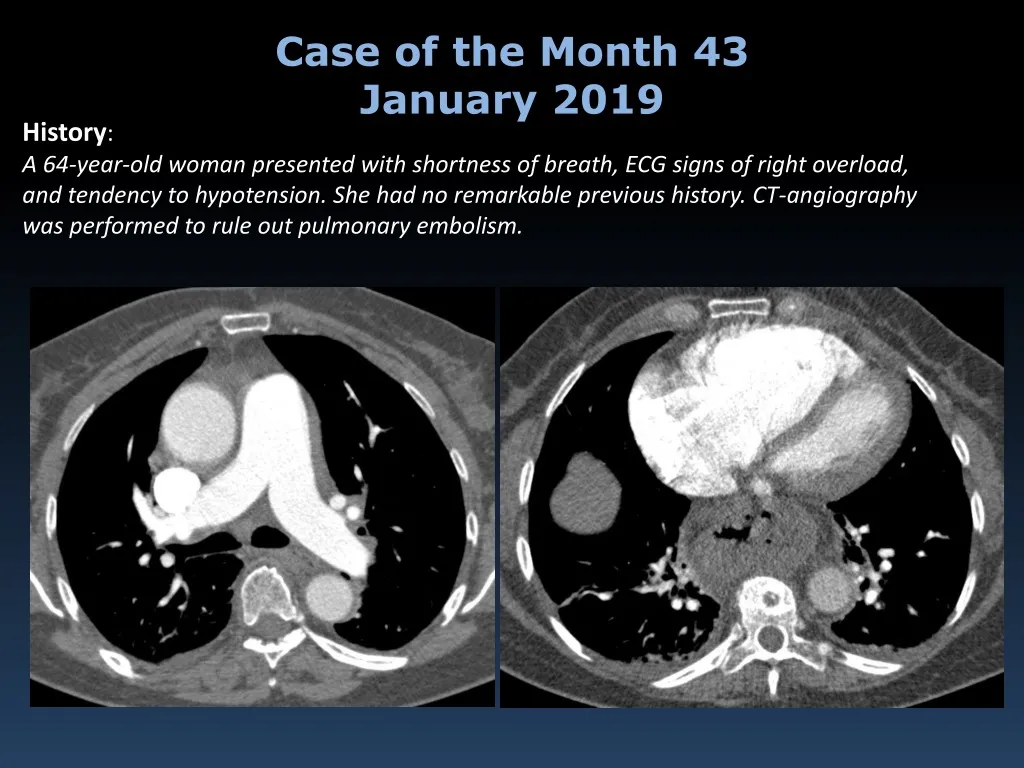
Case of the Month 43 January 2019. History : A 64-year-old woman presented with shortness of breath, ECG signs of right overload, and tendency to hypotension. She had no remarkable previous history. CT-angiography was performed to rule out pulmonary embolism. Case of the Month 43.

E N D
Case of the Month 43 January 2019 History: A 64-year-old woman presented with shortness of breath, ECG signs of right overload, and tendency to hypotension. She had no remarkable previous history. CT-angiography was performed to rule out pulmonary embolism.
Case of the Month 43 MIP reconstructions
Case of the Month 43 What is your diagnosis ?
Case of the Month 43 January 2019 History: A 64-year-old woman presented with shortness of breath, ECG signs of right overload, and tendency to hypotension. She had no remarkable previous history. CT-angiography was performed to rule out pulmonary embolism. Question: What are the key findings on the CTA?
Case of the Month 43 MIP reconstructions
Case of the Month 43 • Signs of pulmonary hypertension with cardiac repercussion (dilatation of the pulmonary trunk) • Dilatation of right cardiac chambers • (incidental, hiatal hernia)
Case of the Month 43 • Mediastinal lymphadenopathy • sign of malignancy • Centrilobular nodules due to diffuse • vascular tree-in-bud
Case of the Month 43 What is your diagnosis ?
Case of the Month 43 The patient died 3 days after admission and the CTA. An autopsy was performed.
Case of the Month 43 • Histopathological findings of the lung specimens obtained at autopsy showed: • Tumour embolism (black arrow) in the pulmonary arterioles with fibrocellular intimal proliferation (blue arrows). Neoplastic intravascular cells (asterisk). A gastriccancerwasdiscovered.
Case of the Month 43 Diagnosis Pulmonary tumour thrombotic microangiopathy PTTM Authors: M. Costilla, E. Castañer
Case of the Month 43 Discussion • PTTM can occur in patients with widespread cancer, a history of malignant disease, or occasionally as the first symptom of occult malignancy(as is in our case). • Usually considered rare, intravascular pulmonary metastases are commonly seen at autopsy, particularly in patients with breast, stomach, liver, kidney, lung, or prostate cancer or choriocarcinoma. • PTTM causes increased pulmonary vascular resistance, resulting in severe clinical manifestations: • -new onset or worsening of dyspnoea • -pulmonary hypertension • -right-sided heart failure with cor pulmonale • -sudden death • The radiologic diagnosis of PTTM is difficult because the findings are often minimal or nonspecific.
Case of the Month 43 Discussion • PTTM causes a vascular tree-in-bud sign in the CT; MIP reconstructions are essential to show dilations of the distal pulmonary arteries. A feature that helps in the differential diagnosis with tree-in-bud due to bronchial disease is the lack of changes in the bronchi. • The presence of signs of malignancy and signs of pulmonary hypertension (dilation of central pulmonary arteries and repercussion in the right heart chambers) associated with the vascular tree-in-bud sign are the key for the diagnosis.
Case of the Month 43 Discussion • PTTM should be considered in the differential diagnosis of acute/subacute cor pulmonale, and PH in patients with known cancer and in those without. • MIP reformations are essential to visualize the vascular tree-in-bud. • The accompanying signs of malignancy provide a clue to the diagnosis. • Differential Diagnosis • Bronchial causes of the tree-in-bud pattern • Other vascular causes of tree-in-bud: • Excipient lung disease, related to intravenous injection of substances containing filler material (insoluble excipients such as starch, cellulose, or talc). • Other causes of pulmonary hypertension
Case of the Month 43 Further Reading PULMONARY TUMOUR THROMBOTIC MICROANGIOPATHY 1) Franquet T, Giménez A, Prats R et al. ThromboticMicroangiopathyofPulmonaryTumors: A Vascular Cause of Tree-In-Bud Pattern on CT. AJR 2002;179:897-899. 2) S.Miyano, S. Izumi, Y. Takeda et al. Pulmonary tumor thromboticmicroangiopathy. J. Clin. Oncol. 2007; 25: 597-599. 3) Chinen K, Tokuda Y, Fujiwara M et al. Pulmonary tumor thromboticmicroangiopathyin patients with gastric carcinoma: An analysis of 6 autopsy cases and review of the literature. Pathology - Research and Practice 2010; 206: 682-689. 4) Price LC, Wells AU, Wort SJ. Pulmonary tumour thrombotic microangiopathy. CurrOpinPulm Med. 2016 Sep;22(5):421-8.
















