Download
1 / 54
540 likes | 645 Views
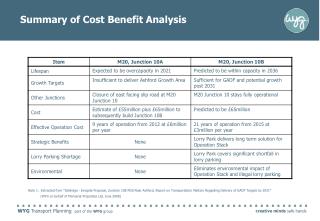
An Analysis of Community Benefit of Montana Hospitals. Presented by: MHA…An Association of Montana Health Care Providers. What should you gain from this?. Better understanding of benefit of community hospital Better understanding of financial impacts of unfunded care

E N D
An Analysis of Community Benefit of Montana Hospitals Presented by: MHA…An Association of Montana Health Care Providers
What should you gain from this? • Better understanding of benefit of community hospital • Better understanding of financial impacts of unfunded care • Greater appreciation for services provided by hospital
Areas of Focus • Unfunded Care • Charity Care • Bad Debt • Government Shortfalls • Economic Impact • Providing more than health care • Education • Future professionals developed today
More than just health care • Montana hospitals play many roles in their communities • Direct service providers • Large employers • Community partners • Sources of volunteers • Educators
Mission Statement According to the 2005 AHA survey, 93% of Montana hospitals have a focus of community benefit in their mission statements.
Caring for the indigent population Charity Care Caring for the uninsured and underinsured Bad Debt and Charity Care Community Education and Outreach Wellness exams Support groups Immunization programs Clinics Patient Education Types of Community Benefit
Charity Care • Care provided for people who do not have the means to pay. • “The giving of services because of human need regardless of ability to pay.” Dennis O’Malley, Craig Hospital
Rural Charity Care Charity Care figures from Annual AHA survey for Montana hospitals.
Urban Charity Care Charity Care figures from Annual AHA survey for Montana hospitals.
Statewide Charity Care Charity Care figures from Annual AHA survey for Montana hospitals.
What This Means… • MT Statewide, a 248% Increase in 9 years for Charity Care • $17.1 M in 1997 • $59.5 M in 2005 • What is causing this increase? • Increase in health care costs • Decrease in employer coverage
Programs Can Be Affected by Increasing Charity Care • When charity care burdens are too high, other community benefit programs may have to be reduced in scope or curtailed. • A facility may have to reduce services that don’t pay their own way to preserve the core services valued by the community.
Public Misconceptions About Charity Care • “It’s their own fault. It’s not my problem.” • Charity care patients are just too lazy to get insurance or a job • Often labeled as “no-goods” • If you walk into the emergency room, you will get treated even if it’s not an emergency • This is changing in many facilities
Truths About Charity Care Patients • Many patients face “health care versus food” • Charity care patients often barely make enough to survive without health care costs • The majority of the uninsured and underinsured have jobs but no employer coverage
What is Bad Debt? “The uncollected charges for care to patients who are believed to have the financial ability to pay at the time the care is provided, but don’t pay.”
Bad Debt continued… Bad Debt figures from Annual AHA survey for Montana hospitals.
More Bad Debt… Bad Debt figures from Annual AHA survey for Montana hospitals.
Bad Debt Statewide Bad Debt figures from Annual AHA survey for Montana hospitals.
% Increase in Bad Debt at Every Level (1997-2005) • 150% - Urban • 105% - Rural • 142% - Statewide
Insurance premiums continue to rise Employers can not cover premium Leaves patient with greater expense Self –employed and part-time employees can not afford premiums In 2006, one typical health insurance policy in MT cost $1,435/yr for healthy 25 year old and $2892 for a healthy 55 year old, but each faces a $5,000 deductible. Cause Effect
Insurance and government program regulations are becoming more strict - i.e.: patient is allowed one colonoscopy per year Patients who are concerned about their health end up paying out-of-pocket for additional procedures Working poor do not qualify for Medicaid Not enough money in CICP to cover everyone Cause Effect
Contrary to Popular Opinion… In 2003, more than 80% of all uninsured adults nationally whose incomes fell below 200% of federal poverty level were deemed ineligible for Medicaid and other public health insurance programs Who’s Uninsured in Colorado and Why?, Families USA, November 2003
Single person $9,800/year $19,600/year (200%) Two person family $13,200/year $26,400/year (200%) Family of three $16,600/year $33,200/year (200%) Family of four $20,000/year $40,000/year (200%) Federal Poverty Level 2006
Thoughts from Around Montana • “A better informed public and a willingness on their parts to access care as appropriately as possible could make for a healthier population and the potential for reducing some bad debt.” Kay Wagner, Patient Business Services, St. Vincent Healthcare. • “Our bad debt expense has grown significantly in the past few years, and finding a workable solution is a top priority.”Kim Lucke, Director of Finance, Northern Montana Hospital • “With the increase in the number of patients that are uninsured and underinsured, hospitals must be "creative" in the collection of Accounts Receivable to manage bad debts. Hospitals are sensitive to people paying their medical bills; however, hospitals must collect for payment of medical services to ensure financial viability and maintain quality services.” Jim Shelton, Manager, Patient Business Services, Benefis Healthcare
Total Uncompensated Care • Combination of charity care and bad debt • Generally grouped together • Difficult to distinguish one from the other
Rural Uncompensated Care Rural Uncompensated Care figures from Annual AHA survey for Montana hospitals.
Urban Uncompensated Care Urban Uncompensated Care figures from Annual AHA survey for Montana hospitals.
Statewide Uncompensated Care Statewide Uncompensated Care figures from Annual AHA survey for Montana hospitals.
What Can be Done to Reduce Uncompensated Care? • Lobby local, state and federal governments for increased allocations • Increased endowments and contributions from community groups • Continued consumer education regarding over-utilization and abuse of health care system • Not using Emergency Department as primary care for non-emergencies • Increased coverage by employers/insurance reform • Include part-time employees under coverage • More affordable to small businesses
MEDICARE Federal program Larger, general acute care hospitals are paid at a predetermined rate for 511 categories of illness Payment is same for each patient within specific category no matter the level of care provided Critical Access Hospitals are paid 101% of their reasonable costs. MEDICAID State program Larger, general acute care hospitals are paid at a predetermined rate for 511 categories of illness Payment is same for each patient within specific category no matter the level of care provided Critical access hospitals are paid 101% of their reasonable costs. Government Programs
Medicare and Medicaid Shortfalls Shortfall – difference between what the hospitals charge for services and the payment received for care given
Rural Medicare/Medicaid Shortfalls Rural Medicare & Medicaid figures from Annual AHA survey for Montana hospitals.
Urban Medicare/Medicaid Shortfalls Urban Medicare & Medicaid figures from Annual AHA survey for Montana hospitals.
Statewide Medicare/Medicaid Shortfalls Statewide Medicare & Medicaid figures from Annual AHA survey for Montana hospitals.
Montana Hospitals Help Fund Medicaid Payments • Beginning in 2003 hospitals have paid a fee for each inpatient bed day to help fund Medicaid. • The fees are matched with federal Medicaid dollars to help boost Medicaid payments. • The project has helped reduce the gap between what Medicaid pays hospitals and the cost to provide care to program beneficiaries. • This means lower health costs for other Montanans.
How payment shortfalls can impact patient care • Community programs cease to exist • Cost-shift from hospital to insurance to employer to patient • Hospitals becoming less willing to take Medicare/Medicaid patients • Potential for trauma programs and other facilities to close • Hospitals are becoming unable to expand patient services
Other Community Benefit • Community Programs • Available to all patient populations • Economic Impact • More than “just a paycheck” • Education • Future faces of health care
Community Programs Community programs offered at little or no cost to the patients, will begin to decrease non-necessary hospital visits
Programs Offered by Montana Hospitals • Free/discounted preventive screenings • School-based clinics • Senior companion programs • Free child car seat checks • Prenatal exams for underserved populations
Financial Implications of Community Benefit Programs • Montana hospitals provide steep price discounts to support the CHIP program. Lower prices means more children can obtain coverage. • Many programs throughout the state are big money losers but hospitals continue to provide them as best they can. • Hospitals are becoming the primary access point for more low income Montanans.
Employment Benefit • Hospital jobs benefit more than just their employees • Nationally, hospitals support one out of nine jobs in US directly or indirectly • Each of those hospital jobs supports about two additional jobs
MT Employment Benefit Source: Research & Analysis Bureau, MT Department of Labor & Industry, QCEW program.
Continued employment benefit Total Employment Impact of Montana’s Hospitals Jobs from Hospitals Hospital Employment 20,962 Jobs created in other businesses 16,560 TOTAL JOBS 37,522 Source: Research & Analysis Bureau, MT Department of Labor & Industry, QCEW program.
Montana Hospitals Employment • Hospitals employ 20,962 people. • Hospitals employ many professional staff. Most employees have college educations and advanced degrees. • The average hourly wage in Montana is between $25 and $26 per hour. (Hospital wage index) • Many hospitals are one of the primary employers in the community (generally second to school districts) • In 2002, every hospital job in Montana created or supported 2.5 jobs in other businesses1 • “Impact of Community Hospitals on US Economy, All States and Total US Based on 2002 AHA Annual Survey Data TrendWatch. American Hospital Association. Vol. 6, No. 1. May 2004
Trickle Down Effect • Buy Locally • Construction • Linen processing • Food services • Banking services • Employee spending • Grocery store • Entertainment • Retail store
Added Economic Impact • Not-for-profit hospitals • Tax-exemption allows money to be put back into facility for continuation of services • For profit subsidiaries pay state, local and federal taxes • Statewide Hospital Expenditures • $1.5 billion in expenditures translates to $3.75 billion effect on total state economy