Download
1 / 56
570 likes | 749 Views
Prevention of dementia Leon Flicker Western Australian Centre for Health & Ageing, Western Australian Institute of Medical Research, University of Western Australia Royal Perth Hospital. Overview.

E N D
Prevention of dementia Leon Flicker Western Australian Centre for Health & Ageing, Western Australian Institute of Medical Research, University of Western Australia Royal Perth Hospital
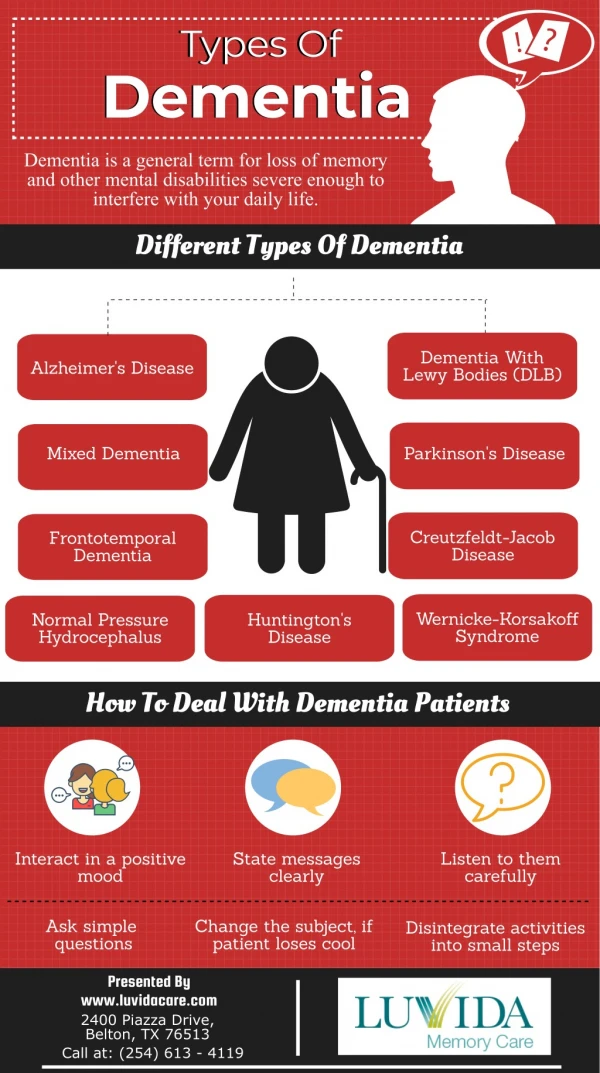
Overview • Why prevention of cognitive decline and dementia are important but recent assistance provided by the NIH has been counterproductive • Antihypertensives and 6 lifestyle influences • Physical activity • Education & cognitive stimulation • Social engagement • Smoking • Diet • Alcohol
What would happen if there is a constant improvement in life expectancy? Men Women
Projected populations – pyramid to coffin? Not just an increase in life expectancy but migration!
Global prevalence of dementiaFerri et al, Lancet 2005; 366:2112
Small strokes are a frequent accompaniment of ageing. Whether these strokes produce significant cognitive impairment is debatable. Recent studies indicate that leukoariosis is associated with definite and perceptible changes in memory. AD and VD may share other risk factors in addition to ageing such as systolic blood pressure. Midlife systolic BP has been shown to be associated with cognitive decline, decreased brain volume, and increased white matter hyperintensities. This suggests that chronic high blood pressure may have consequences that are not limited to cerebrovascular disease. Alzheimer’s Disease & Vascular Dementia - Are they distinct diagnoses?
The “Alzheimerization” of dementia • This is the idea that dementia is nearly all due to Alzheimer’s Disease • There are comparatively little data to support this. • Reports have increasingly found less correlation of Alzheimer pathology with dementia than the original report, Blessed et al Br J Psych 1968; 114:797
Association between quantitative measures of dementia and of senile change in the cerebral grey matter of elderly subjects Blessed et al B J Psych1968; 114:797
Age, neuropathology and dementiaSavva et al N Engl J Med 2009; 360:2302The association between the presence of dementia and Alzheimer pathology decreases with age
It is often said (by all sorts of commentators some of whom should know better) that dementia is an unavoidable consequence of ageing. Preventing Dementia – An Unobtainable Goal?Wrong!
Conclusions from the NIH (2010) • Currently, firm conclusions cannot be drawn about the association of any modifiable risk factor with cognitive decline or Alzheimer’s disease. • Highly reliable consensus-based diagnostic criteria for cognitive decline, mild cognitive impairment, and Alzheimer’s disease are lacking, and available criteria have not been uniformly applied. • Evidence is insufficient to support the use of pharmaceutical agents or dietary supplements to prevent cognitive decline or Alzheimer’s disease.
NIH Suggestions for Future Research • For example, ongoing studies including (but not limited to) studies on antihypertensive medications, omega-3 fatty acids, physical activity, and cognitive engagement may provide new insights into the prevention or delay of cognitive decline or Alzheimer’s disease. • Large-scale population-based studies and RCTs are critically needed to investigate strategies to maintain cognitive function in individuals at risk for decline, to identify factors that may delay the onset of Alzheimer’s disease among persons at risk, and to identify factors that may slow the progression of Alzheimer’s disease among persons in whom the condition is already diagnosed.
There are three main considerations in evaluation of interventions in the prevention of dementia. Efficacy Risks or side-effects, cost. These three facets will determine whether the intervention will eventually be made available universally, or targeted at a high risk group. Universal or Targeted?
We will develop a series of interventions which will be effective, cheap and these interventions will not be prone to side-effects. We will then provide these interventions universally e.g. BP treatment, vitamins, physical activity, smoking cessation, cognitive stimulation…. The major disease process causing dementia is a single disease process, called Alzheimer Disease. This disease process has a stable pathogenic pathway with specific inhibitors. It is thus possible to devise a specific strategy to target those individuals who are highly likely to develop the disease. Spectrum of Possibilities
40 42 The Alzheimer Amyloid Precursor protein (APP) - processing … and AD relevant Aß42 may be generated a Aß p3 amyloidogenic non amyloidogenic
The NIA and Alzheimers Association convened three separate working groups to “address recent advances in AD” http://www.alz.org/research/diagnostic_criteria/
The Evidence Free Zone What is happening here
Anti-hypertensives • A recent systematic review (Peters et al, HYVET-COG Lancet Neurol 2008; 7:683–9) included one additional randomized trial to the Cochrane meta-analysis and demonstrated a 13% reduction in the rate of incident dementia with the use of anti-hypertensives. • This may be the best evidence that we will ever obtain on this subject due to the bias to the null hypothesis because of the large number of control subjects who require treatment with antihypertensives • The experience from the HYVET study that these trials are no longer able to be performed in the developed world because of the understandable reluctance of clinicians to randomize hypertensive older people to placebo.
Physical Activity • Laurin et al. (2001) explored the relationship between physical activity and cognitive impairment in 4615 community dwellers participating in the Canadian Study of Health and Aging who were followed-up for 5 years. High activity levels were associated with reduced risk of cognitive impairment (OR=0.58, 95% CI 0.41-0.83), AD (OR=0.50, 95% CI 0.28-0.90), and dementia of any type (OR=0.63, 95% CI 0.40-0.98).
Systematic review of physical activity and dementia Hamer and Chida Psychological Medicine 2009 39:3
Cochrane Review (Angevaren M et al 2008) Mean Duration 14 weeksPhysical activity and enhanced fitness to improve cognitive function in older people without known cognitive impairment (up to 12/05) Visual Attention
0 6 12 18 Monitored Unsupervised Fitness for the Ageing Brain Study Lautenschlager et al JAMA 2008; 300:1027 n= 170 RCT Usual activity Control Unsupervised WALK or activity Exercise Time (Months)
Effect of Physical Activity on Cognitive Function in Older Adults at Risk for Alzheimer’s Disease: Randomized Trial. Lautenschlager et al JAMA 2008; 300:1027
Fitness for the Ageing Brain Study • Conclusions • The intervention resulted in 142 min more physical activity per week (20 min per day or 9000 steps/week) compared to usual care. • The improvement on the ADAS cog score is modest, 1.3 points on the ADAS-cog but remarkable considering the amount of physical activity undertaken. • The benefits were apparent after 6 months and persisted for at least another 12 months after the end of the supervised intervention. • The intervention is simple and safe. • Physical activty is a modifiable lifestyle factors which might be able help to delay the clinical onset and progression of cognitive decline.
In a longitudinal cohort study of 801 older Catholic nuns, priests and brothers without dementia, cognitively stimulating activities were documented at baseline and the cohort followed-up for 4.5 years (Wilson et al., 2002). A 1-point increase in the cognitive activity score was associated with reduced decline in global cognition (by 47%), working memory (by 60%) and perceptual speed (by 30%), and a 33% reduction in the risk of AD (hazard ratio, 0.67, 95% CI 0.49-0.92). Cognitive reserve or protection (future proof)? Education & Cognitive Stimulation
Predicted 12-year paths of change in global cognition in persons with 8, 12, or 16 years of education (Chicago Health and Aging Project Wilson et al 2009) Cognitive Reserve?
Cognitive Stimulation • The effect of cognitive training on normal older people has also been reviewed (Valenzuela & Sachdev AJGP 2009) . • Seven studies were included in the meta-analysis with six of these studies using neuropsychological tests as the main outcomes. • There were positive results seen in these studies but the results of these neuropsychological tests in normal older people are difficult to extrapolate to everyday function or to prevention of dementia.
Here we report the results of a six-week online study in which 11,430 participants trained several times each week on cognitive tasks designed to improve reasoning, memory, planning, visuospatial skills and attention. Although improvements were observed in every one of the cognitive tasks that were trained, no evidence was found for transfer effects to untrained tasks, even when those tasks were cognitively closely related
Social engagement • It has been demonstrated that rodents reared in “enriched” environments have enhanced cognitive abilities in spatial and non spatial memory tests and enhanced hippocampal neurogenesis . • In humans some studies found no association whereas associations were founds with diverse factors, e.g. social disengagement, emotional support, social and “productive” activities. • Six studies examined the association between social networks and the onset of dementia, the studies often found diverse associations. E.g. The relationships studied included never married as opposed to number of social contacts or quality of social networks.
SMOKINGSummary of selected case-control studies looking at the association between ever smoking and AD. Favours smoking Favours not smoking
Summary of selected cohort studies looking at the association between ever smoking AD Favours smoking Favours not smoking
Smoking Is Associated With Reduced Cortical Regional Grey Matter Density In Brain Areas Associated With Incipient Alzheimer’s Disease Smokers showed decreased grey matter density relative to controls in the posterior cingulate and precuneus (Figure A), as well as the left parahippocampal gyrus (Figure B).
Largely we rely on observational data The effect of micronutrient supplements may not be the same as that obtained from foodstuffs Vitamin E supplements in high doses may have risks and no micronutrient has been demonstrated in RCT to prevent dementia. Saturated fat may also have risks, possibly associated with obesity. What we drink may also be good for us!! SummaryWe are what we Eat!
Baseline and Changes of Hcy at 24 months for the intervention and placebo groups
Changes in Aβ1-40 over 24 months (pg/ml) There have been 2 recently reported studies, one +ve and one -ve, examining cognitive outcomes with tHcy lowering supplements
A Controlled Trial of Homocysteine Lowering and Cognitive Performance NEJM 2006; 354: 2764
Homocysteine-Lowering by B Vitamins Slows the Rate of Accelerated Brain Atrophy in Mild Cognitive Impairment: A Randomized Controlled Trial (Smith et al 2010 PLoS ONE 5:9) • The mean rate of brain atrophy per year was 0.76% [95% CI, 0.63–0.90] in the active treatment group and 1.08% [0.94–1.22] in the placebo group (P = 0.001).
Results of prospective studies of antioxidants as a protection factor for AD, dementia or cognitive decline (Jorm 2002)
Mortality of low and high dose Vitamin E Miller, E. R. et. al. Ann Intern Med 2005;142:37-46