Download
1 / 55
620 likes | 950 Views
Femoracetabular Impingement: In Theory and In Practice. Tom Bradbury, MD Assistant Professor Emory Orthopaedics and Spine Center. March 11, 2011. A delay in non- arthroplasty treatment options for the hip……. Hip pain in the young patient not as common

E N D
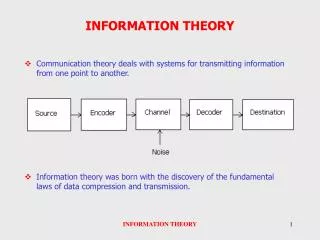
Femoracetabular Impingement: In Theory and In Practice Tom Bradbury, MD Assistant ProfessorEmory Orthopaedics and Spine Center March 11, 2011
A delay in non-arthroplasty treatment options for the hip……. • Hip pain in the young patient not as common • Hip is “deeper” than knee, shoulder • Hip is more constrained • Hip capsule is very robust • Precarious blood supply to the femoral head limited an interest in surgical exposure…a fear of iatrogenic avascular necrosis
“90% of adult cases of osteoarthritis are the result of a morphologic developmental abnormality”…..not a intrinsic problem with articular cartilage • Murray, 1965 • Harris, 1986
“Structural Pediatric Residuals” • Developmental Dysplasia • Slipped Capital Femoral Epiphysis • Legg-Calve-Perthes Disease • Multiple Epiphyseal Dysplasia • Spondyloepiphyseal Dysplasia
Radiography of Hips with FAI • Normal joint space • Subtle morphologic aberrations “Normal” to the untrained eye
1991: “cervico-acetabular impingement” secondary to femoral neck malunion • 1999: “pincer” type impingement after periacetabularosteotomy for dysplasia
Evolution of an Understanding • Reinhold Ganz • Anatomy • Perfusion • Osteotomy • Dislocation • Impingement
Ganz’s Observation “Overcorrection” of hip dysplasia with periacetabularosteotomy “Iatrogenic retroversion” Hip pain with flexion (Pincer type anterior impingement)
Normal Cam Pincer
Hip “History” Arthrosis • Insidious onset • Constant Ache • Walking on level ground • Nocturnal symptoms Pre-arthrosis • Sudden onset • Sharp, intermittent pain • Pain primarily with torsional activities • Pain with prolonged flexion
Hip Exam: Gait • “Antalgic” – shortened stance phase secondary to pain • “Trendelenberg” – contralateral hip drops during stance phase secondary to abductor dysfunction • “Abductor Lurch” – torso sways over affected leg during stance phase secondary to abductor dysfunction
Hip Specific Tests • Trendelenberg Test • Log Roll • Passive External Rotation in Extension • “C” test • Thomas Test • Stinchfield Test • Ober’s Test • Anterior Impingement Test (FADDIR) • Posterior Impingement Test • DEXTRIT (aka McCarthy)- Dynamic External Rotatory Impingement Test • DIRIT- Dynamic Internal Rotatory Impingement Test • Scour Test • Ober • Abduction internal rotation • FABER
Hypermobility • Beighton’s Criteria for hypermobility (3 of 5) • Thumb to forearm • SF extension > 90 • Elbow hyperextension > 10 • Knee hyperextension > 10 • Palms to floor
Findings • Drehmann’s Sign- Obligate abduction and external rotation with forward flexion of the hip • CoxaSaltansInterna- Iliopsoas tendon over the ileopectineal eminence • CoxaSaltansExterna- Iliotibial band over greater trochanter
Imaging of the Young Hip Start with plain films: • Supine AP Pelvis Centered Low with Legs internally rotated 15 degrees • Cross table lateral of the hip with the leg 15 internally rotated 15 degrees • Dunn 45 of the Hip
Technique: • AP • Supine with legs 15 degrees internally rotated • Film-focus distance: 1.2 meters • Point of center: midway between ASIS & Pubis • Cross Table Lateral • Leg 15 degrees internally rotated • Perpendicular to long axis of femoral neck
Technique • Dunn 45 • Hip flexed 45 degree, abducted 20, in neutral rotation
“Diagnosis can only be made from a technically sound and properly positioned AP radiograph of the pelvis” -Ganz
Distance from tip of coccyx to superior edge of symphasis? 1 – 3 cm Siebenrock et al. From Sacrococcygeal junction: Male = 47.3 mm Female = 32.3 mm TILT?
ASIS PUBIS POINT OF CENTER?
Ilioischial Line Iliopectineal Line
Posterior Wall Anterior Wall
Hip Imaging Lingo • Acetabular Depth • Acetabular Extrusion • Acetabular Inclination • Femoral Head Coverage • Acetabular Version • Head Sphericity • Head-Neck Offset • Congruency
Acetabular Depth • The relationship of the true floor of • the acetabulum to the ilioischial line • Extrusion Index
Extrusion Index E/A+E Normal = 25% A E
Cox Profunda • Floor of fossa medial • to ilioischial line • - Extrusion Index 0
Cox Profunda • Floor of fossa medial • to ilioischial line • - Extrusion Index 0
AcetabularProtrusio • Femoral head to ilioischial line • Negative Extrusion Index
Acetabular Inclination (Tonnis angle) • Horizontal line between center of femoral heads • Line connected the medial and lateral edge of the • sourcil
Acetabular Inclination (Tonnis angle) Negative angle = overcoverage/pincer
Acetabular Inclination (Tonnis angle)High positive angle = dysplasia
Lateral Center Edge Angle (of Wiberg) • Normal = 25 - 40
Sphericity • Measured by containment of physeal scar with circle of femoral head
Acetabular Version • Relationship of walls to one another • Ischial spine within pelvis • Relationship of posterior wall • to center of femoral head
Dysplasia • Low CE angle (< 25) • Elevation of acetabular inclination • Elevation of Extrusion index
RetrovertedAcetabulum • Cross over sign • Ischial Spine within pelvis
False profile view Posterior Anterior
Aspherical head • Physeal Scar extends beyond • the circle
Femoral Cam • Alpha angle > 50